8-8:30) How to have difficult conversations – Dr. Keith Baker, MD
- Make sure you have the time for these conversation
- Make sure you have someone with you when you break the news
- Positioned in the room in an area where you can get out
- Opening line “what do you know that’s going on” or “I am sorry I have some difficult news for you” or something
- In a brief way step them through what actually happened
- “ I am very sorry she or he has Died” you have to say it …. Then you stop talking
- If you feel comfortably you can give family hug ect
- “Is there anyone you need us to call for you”
- “Do you want a chaplan here?”
- “ if you have any questions we are here for you”
8:30-9) Who are the immunosuppressed?- Patrick Cheatle, MD
- Immunosuppressed
- Autoimmune
- Transplant recipients
- Chronic conditions requiring steroids
- Cancer patients
- Immunosuppressive medications
- Corticosteroids
- Calcineurin inhibitors
- Antimetabolities
- Immunoglobulins
- Ionizing radition
- Biologic alkylating agents
- Glucocorticoids- suppress antibody complement binding; inhibits synthesis of all inflammatory cytokines
- Side effects:
- increased susceptibility to infection
- Impaired wound healing
- Hyper glycemia
- Htn
- PUD
- Psychiatric stuff
- Osteopenia
- Weight gain
- Side effects:
- Glucocorticoids withdrawal
- Can suppress HPA but needs to be on it for over 3 weeks.
- Wd symptoms looks like adrenal insufficiency
- If they are on them over 3 weeks then they need a taper
- Calcineurin inhibitors- tacrolimus, cyclosporine
- Inhibit calcineurin suppress t and b cells
- Most post transplant patients on it
- Calcineurin inhibitors Side effects
- Nephrotoxic
- Htn
- HyperK
- Hypomag
- Neuro shit
- Antimetabolitis MMF
- Inhibit proliferation of T and B lymphocytes
- Chemo agents and organ transplants
- Side effects
- Bone marrow suppression
- GI stuff
- Immunoglobulins
- Monoclonal antibody that binds to CD52🡪 targets lymphocytes for destruction
- CLL and MS treatment
- Transplant patients
- Lifelong immunosuppression
- Adverse outcomes are directly proportional to increasing age of the recipient and donor organ
- Infections in transplant recipents
- <1 month s
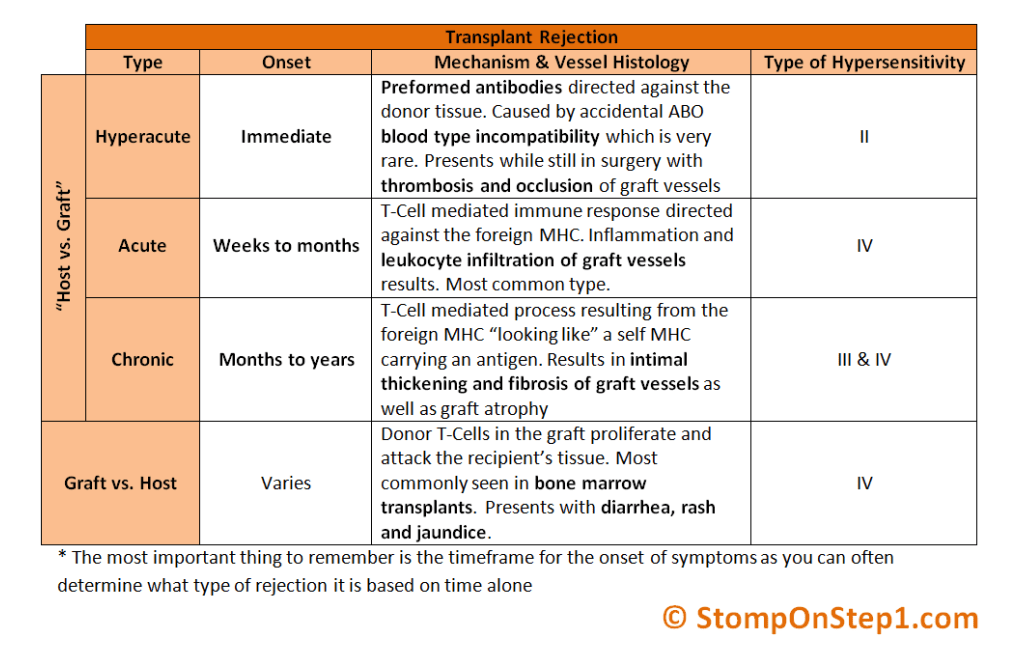
- Rejection time lines

- GVHD TX
- Tx:
- glucocorticoids; high dose
- Calcineurin inhibitors
- Empiric abx
- Tx:
9-9:30) Airway review – John Pester, DO
- Pester showed us videos of our intubations with the new glidescope gave us pointers on how to improve
- ALWAYS HAVE EPIGLOTTIS IN THE VIEW if you do not see it then you went tooooooo far.
- C collar patients- always use hyper angulated blade (S3)
9:30-10:30) Interactive Board Review – Rachel Patterson, MD
- Pictionary
10:30-11) Mentorship – Rebecca Jeanmonod, MD
- Humanism – learning, science on how people learn and grow
- Knowing – action – meaning
- Humanism – fulfillment of purpose.
- What makes a good teacher – being an example, patience, empathy
- Mentorship – beyond the classroom
- Longterm, profession and personal growth, focus on development, dyad, subject agenda, informal, structured
- Real, acceptance, empathy, needs assessment, goals,
- Listen — ask —advise
- Seeing potential
- Support from below, place protection
11:00-11:30) EM Case Presentation – Daniel Greco, DO
11:30-12) TRIAGE – Chiefs
- Toxicology
- Isoniazid toxicity: TRIAD
- Refractory seizures
- SEVERE metabolic acidosis
- Coma
- TX: B6
- Isoniazid toxicity: TRIAD
- Radiology

- Kartagener syndrome-sinus inversous primary ciliary dyskinesisa ( infertility stuff and lung stuff)
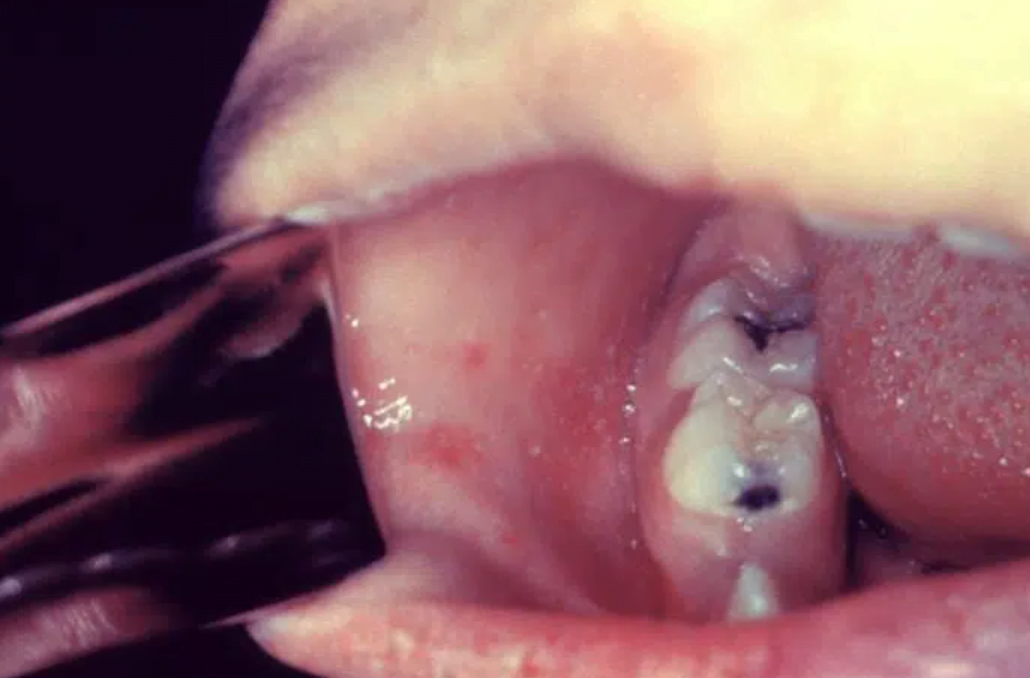
- Integument:

- Koplik spot- lesions on buccal mucosa consisting of pinpoint greys spots surrounded by bright red inflammation.
- MEASLES aka rubeola
- Ancillary
- HOW TO DO PERICARDIALCENTESIS
- AKA please review because instead of TRIAGE we are doing practice this upcoming week.
- https://www.youtube.com/watch?v=GcoAHYcngEw
- https://www.youtube.com/watch?v=OKHOo6m20To
- HOW TO DO PERICARDIALCENTESIS
- General
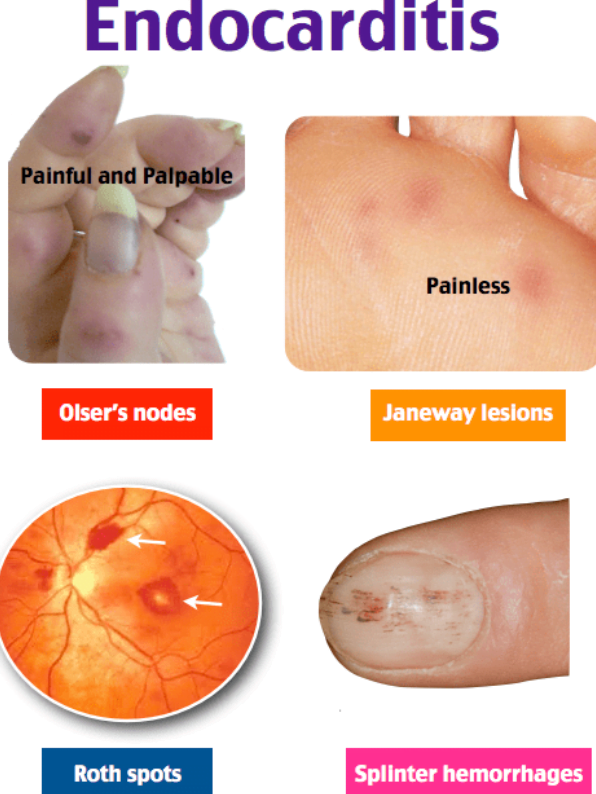
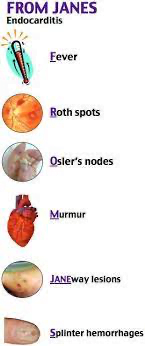
- Endocarditis
- Endocarditis
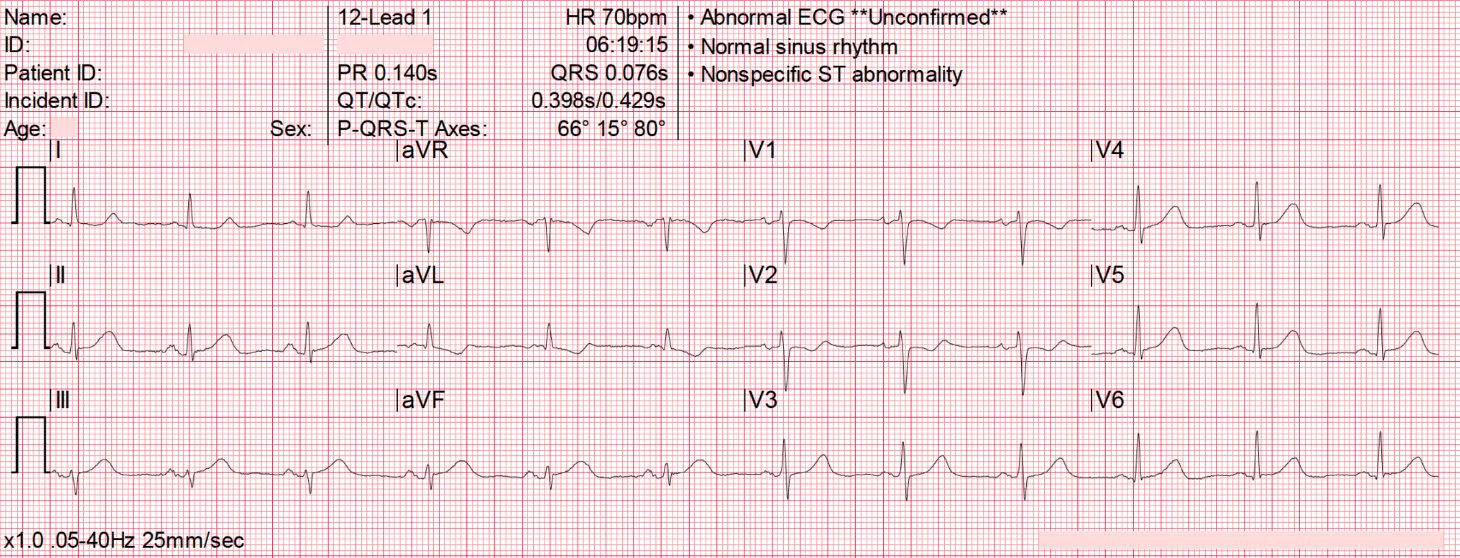
- EKG: 47yoM coming in with cc of nausea
- https://litfl.com/ecg-case-035/

- T waves in leads III and aVF appear to tower over the preceding QRS complex, and have a wide, “bulky” appearance. Such changes are consistent with hyperacute T waves (HATW) representative of hyperacute occlusion and evolving ST elevation
- There is reciprocal ST depression in V1-3 and I
- These changes are suggestive of hyperacute inferior OMI, likely due to occlusion of a dominant RCA given the lack of ST elevation seen in lateral leads. This ECG was faxed from the pre-hospital environment — by the time of arrival to an emergency department it is likely that we would see classical ST elevation evolving.