Valvular Emergencies. Philip Salen, MD
- Mitral stenosis
- MCC Rheumatic fever- autoimmune reaction to GA Strep pharyngitis
- MC school age
- 5 things- JONES-
- Polyarthritis
- Carditits
- Sydenham’s chorea
- Erythema marginatum
- Nodules
- TX: PCN + anti-inflammatory
- MCC Rheumatic fever- autoimmune reaction to GA Strep pharyngitis
- Valve Leaflets
- Endocarditis
- Risk factors: IVDA, valve replacements, HIV, HD
- ESR+CRP+ 3 Blood cultures + echo
- MCC S. Aureus ; strep second mcc
- Later findings
- Osler’s nodes= hurt; tender red
- Jane way lesions= non tender palms
- Splinter hemorrhages
- Veg over 1cm = likely to embolize
- Tricuspid and pulmonic endocarditis 🡪 embolize to LUNG
- Patent foramen ovalue (12%) so then go to brain.
- Mitral and aortic valve endocarditis🡪 brain mc spot
- Roth spots retina
- High risk patients for endocarditis REQUIRE abx ppx prior to
- I&D
- Regional anesthesia for dentalgia
- AMPICILLIN, VANC, AMOXICILLIN
- Endocarditis
- Congenital valvopathies
- MVP – most common
- Most common pathology necessitating heart valve replacement up to 70? Bicuspid
- Above 70- calcifications aortic valve
- AS
- 2nd intercostal space
- Dyspnea, CP, syncope
- Emergent echo
- PE method for estimating the severity of Ao valve stenosis: pulsus parvus et tardus- slow to rise and late peaking
- As valve area severity—Sevre <1cm
- Don’t decrease preload it will make it worse
- Bicuspid aortic valve- risk for aortic dissection higher
- Prosthetic valve surgery 12 months ago-
- What kind of valve and which valve
- Mechanical ( INR 2.5-3.5) warfarin —-(for aortic valves 3-4)
- Metal
- Prosthetic – bioprosthetic don’t need AC after first month. / wear out more frequently
- Porcine
- Bovine
- Human allographs/autographs
- Both can have MRIs
- Mechanical ( INR 2.5-3.5) warfarin —-(for aortic valves 3-4)
- What kind of valve and which valve
- Aortic regurg
- Low pitched Diastolic murmur at the apex, early high pitched blowing diastolic murmur at L sternal boarder, wide pulse pressure, rapid upstroke of carotid
- Wide pulse pressure
- Mitral regurgitation
- Holosystolic
- Pectus extavatum- worry about dissection; marphans or Ehlers Danlos
- Mechanical AoV with dyspnea and near syncope- Crescendo decreshendo🡪 STAT ECHO must r/o endocarditis
- Hemolytic anemia more common in mechanical valves
10:45-11:15) EKG Reading Part 3. Keith Baker, MD
- Rate
- Rhythm
- Axis
- Sinus block
- BBB (What we are covering today)
- Caused by block of conduction in the left or right bundle
- Normally depolarization stimulus is conducted to both ventricles simultaneously
- The block bundle branch delays depolarization to the ventrical that it supplies
- Unblocked ventricle begings depolarizing
- Because one ventricle depolarizes slightly layer then other you get joint ORS🡪 big
- BBB- 3 small blocks 120ms
- If less then 120 but same morphology then incomplete
- Right bundle- V1 V2
- QRS over 120ms
- RsR’ bunny ear pattern in V1-V3
- Slurred S wave in 1, avL and frequently V5, V6
- LBBB- V5,V6
- QRS >120
- Dominant S wave V1
- Broad R wave in 1, avL, V5-V6
- Prolonged R wave V5-V6
- Wanna see discordance!!
- KEEP IN MIND
- Some people get rate dependent BBB
- When someone with BBB has SVT can look like VTACH
- There are other things that can cause LBBB pattern or RBBB pattern.
- RBBB- TCA overdose
- LBBB- Pacemakers

11:15-12:15) Pacing and Pacemakers. Rebecca Jeanmonod, MD
- Need to know vs Nice to know
- Cracking the code
- 1st letter- what its pacing
- A
- V
- O
- 2nd letter- chamber sensed
- Atrium
- Ventrical
- Dual
- none
- 3rd letter- responsed to sensing
- Triggering
- Inhibiting
- Dual
- none
- 1st letter- what its pacing
- AAI
- Firing atria, listening to atria, inhibiting if hears atria firing by self then inhibits.
- SSS or healthy heart like kids with lyme
- Pacemaker
- Pulse generator
- Electronic circuitry
- Lead system
- Endocardium
- VVI
- Atrial dysrhythmia
- Fires ventricles, listens to ventricle,
- Afib/aflutter
- How to do pacemaker
- 120 pacemaker, right IC, float pacemaker
- Dead heart=no balloon up
- Complications
- Infection
- Hematoma
- Problems with leads
- Dislodged leads
- Perforation- MC at RV apex
- Infection
- Tricuspid regurg
- Coiling- Twiddlers syndrome:
- Failure to capture
- Delivery of pacing stimulus without depolarization
- HAVE TO EXTERNALLY PACE-
- Failure to pace
- Absence to deliver a stimulus to the heart
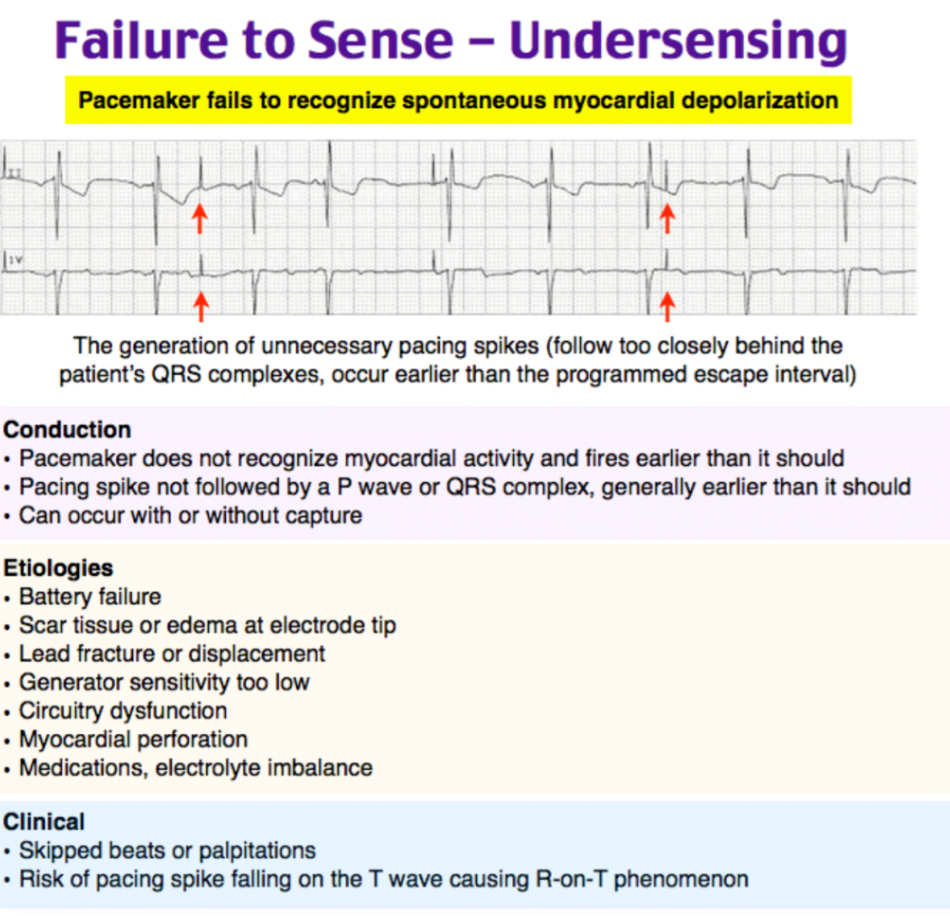
- Failure to sense
- Failure to sense results in paced beat on top of intrinsic beat
- Runaway pacemaker
- Pacemaker mediated tachycardia—only with triggering pacemaker
- Re-entrent SVT looking picture
- Adenosine or magnet
- Magnet- resorts the pacemaker into a backup mode
- Pacemaker syndrome- you feel different
- Atrial stretch🡪 bnp –> CHF
- Pacemaker/ICD infection🡪 Fever, ESR.CRP very helpful
- Pocket complications- vanco
- Head bloating= SVC syndrome, consider DVT
- Cardiac perforation extremely rare
12:40) Triage. Annette Palladino, DO
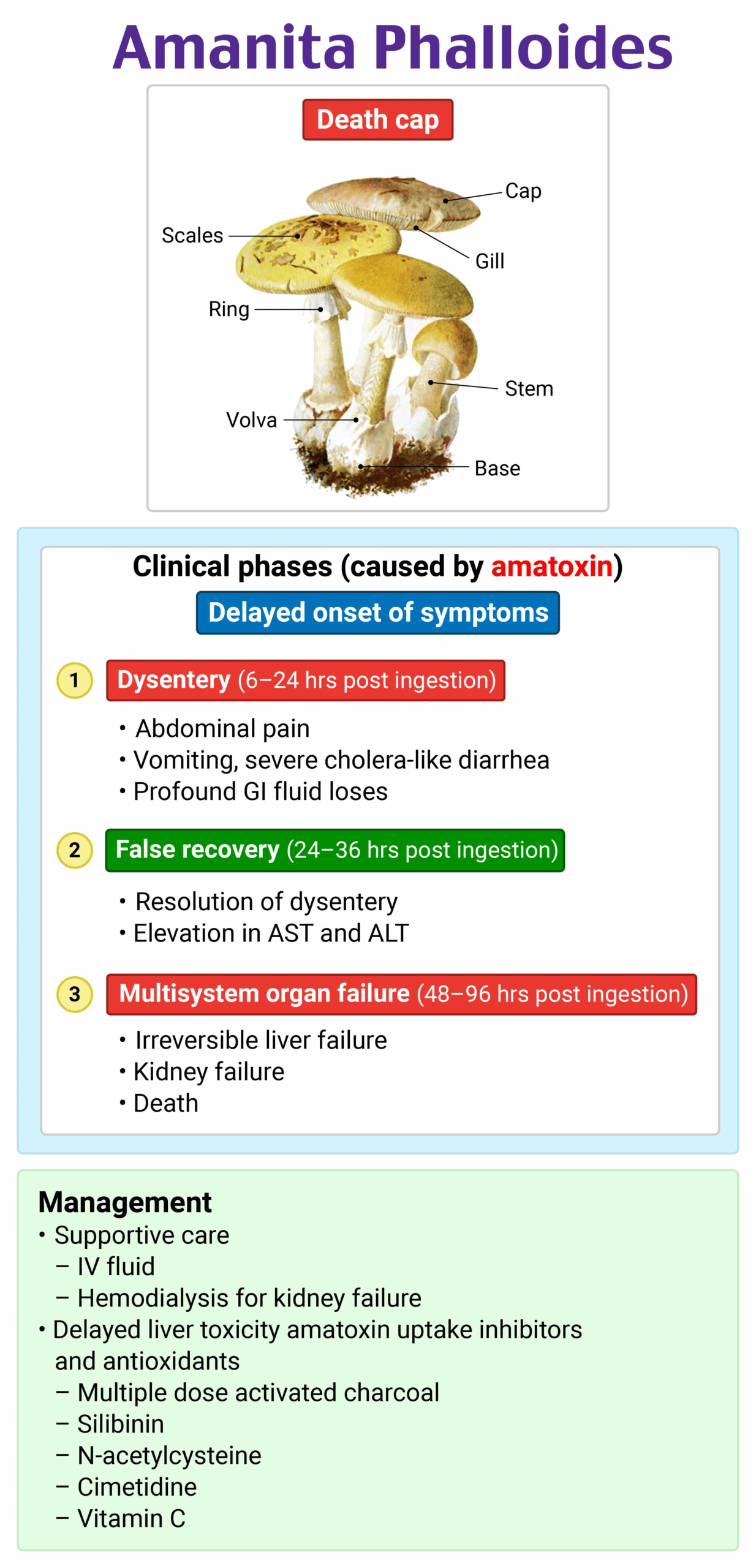
Toxicology
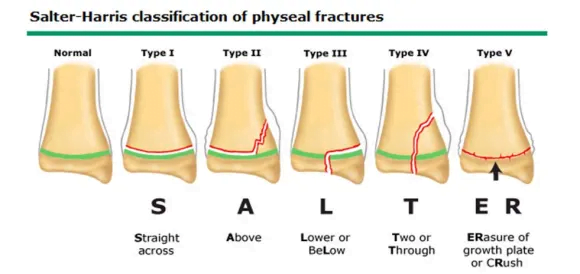
Radiology
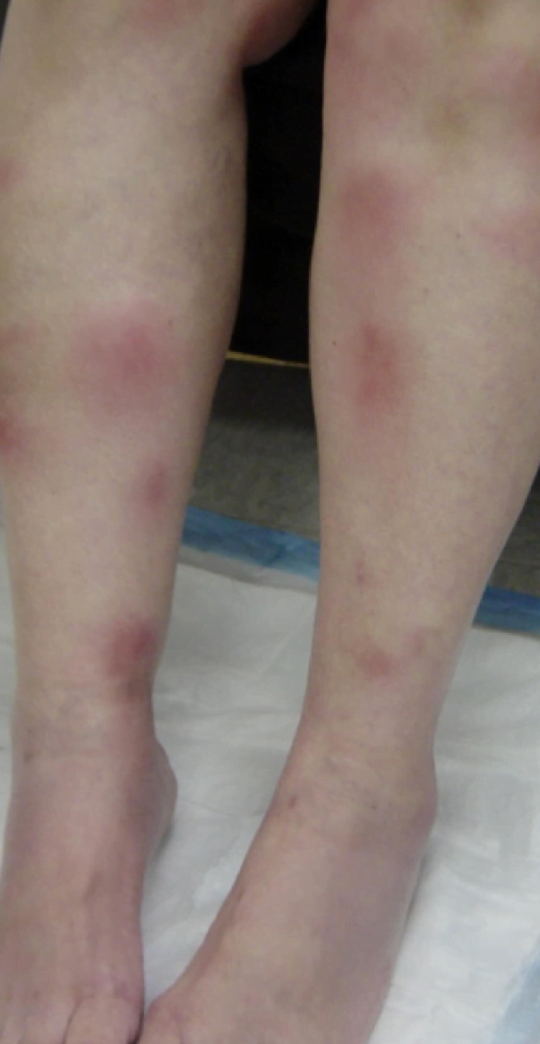
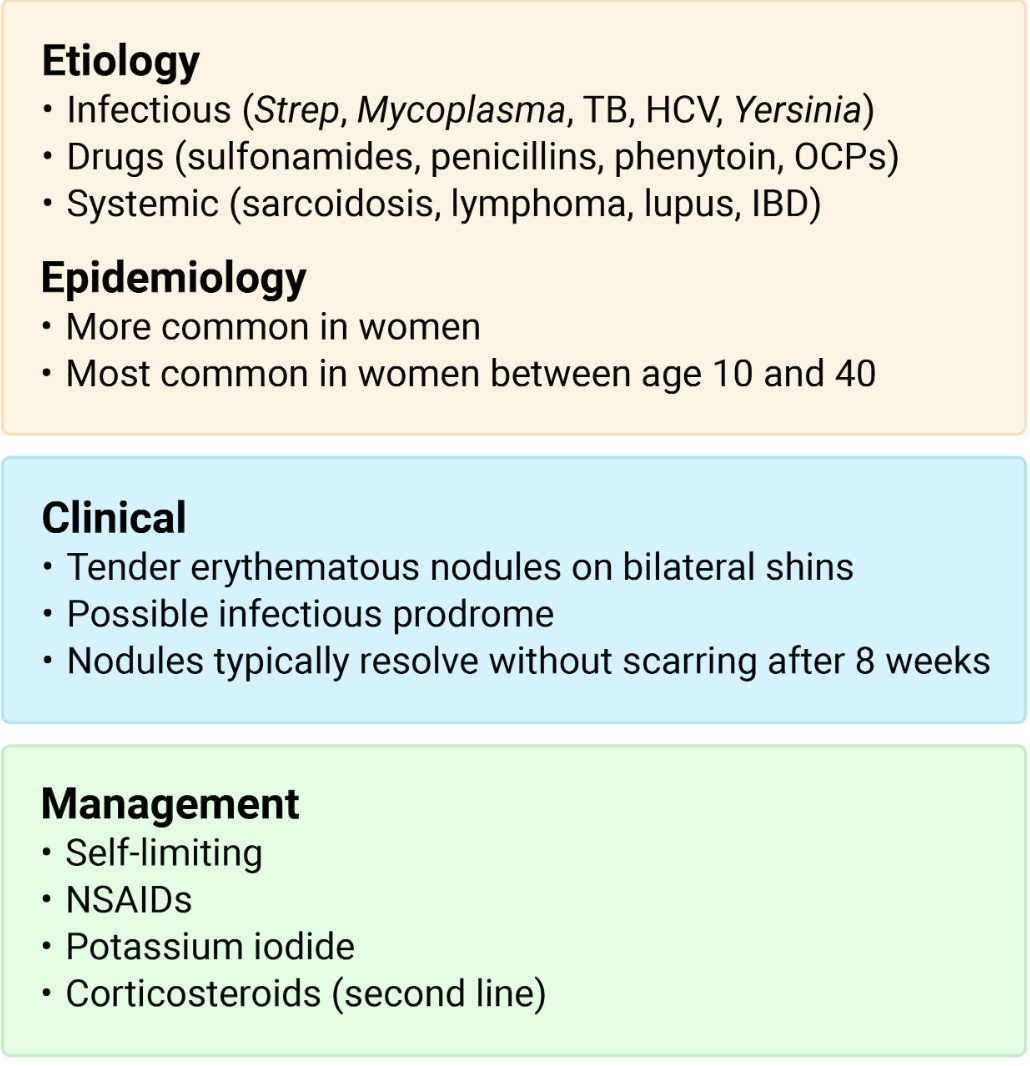
Integument- Erythema Nodosum
Ancillary- TMJ dislocation 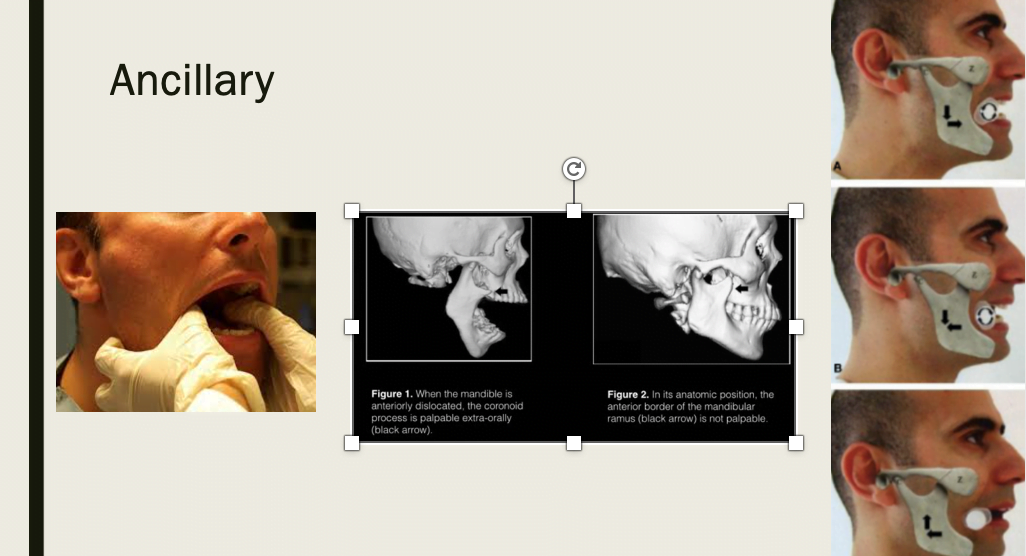
-First, the classic intra-oral approach: this involves the physician placing his/her thumbs into the patient’s mouth along the lower molars, and applying posterior and inferior force to guide the mandible back into its groove, like so:
– Extra-oral technique: When the mandible is dislocated, the coronoid process is palpable externally over the cheek. By applying steady posterior pressure over the coronoid, the mandible can be easily reduced. You’ll know it’s in when the coronoid process is no longer palpable.
– Place a 5 or 10 mL syringe between the patient’s molars on the dislocated side. – Instruct the patient to bite down and roll the syringe back and forth between the teeth until reduction is achieved. – This method utilizes the patient’s own jaw musculature to create the posterior/inferior forces for jaw relocation.
General- OBGY
EKG- Failure to capture