Toxic Alcohols- Dr. Keith Baker, MD
- Ethanol Toxicity
- We know this (:
- Isopropyl Alcohol Toxicity
- Where can I find this?
- Rubbing alcohol, hand sanitizer
- Metabolized by:
- Isopropyl alcohol –ADH🡪 acetone
- Toxicity
- Hemorrhagic gastritis, neurologic
- Hallmark
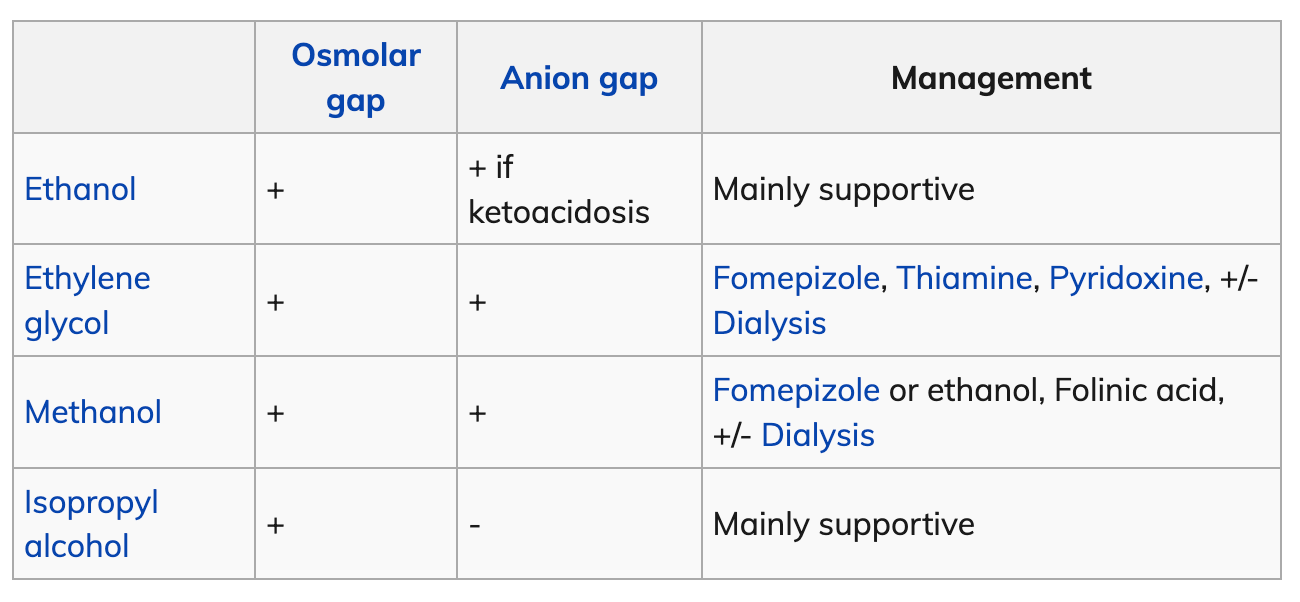
- Osmolar gap, ketosis WITHOUT acidosis
- Lab Pearls
- Serum and urine ketones
- Crt may be falsely elevated due to acetone interference with lab Crt
- Treatment:
- Supportive
- Where can I find this?
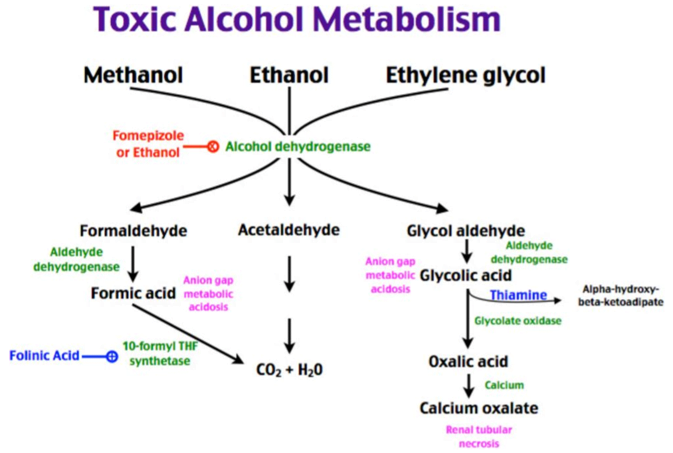
- Methanol Toxicity
- Where can I find this?
- Windshield wiper fluid, De-icing products, Antifreeze, Paint removers
- Metabolized by:
- Methanol —Alcohol dehydrogenase🡪 formaldehyde –aldehyde dehydrogenase🡪 Formic acid
- Formic acid: toxic effects
- Retinal, ophthalmic and neurotoxicity
- What labs should I get?
- Ethanol
- VBG
- What do I see on labs?
- High anion gap metabolic acidosis
- Treatment
- Must block ADH enzyme.
- Fomepizole
- Ethanol
- Correction of metabolic acidosis
- Consider bicarb bolus + infusions
- Dialysis indications:
- Refractory metabolic acidosis ph<7.5 with AG >30
- Renal insufficiency
- Visual symptoms
- Deteriorating vital signs
- Electrolyte abnormalities
- Methanol levels >50mg/dL
- Must block ADH enzyme.
- Where can I find this?
- Ethylene Glycol Toxicity
- Where can I find this?
- Antifreeze- sweet taste
- Buzz word boards: fluoresces yellow/green under woodslamp
- Metabolized by:
- Ethylene glycol –ADH🡪 glycoaldehyde –ALDH🡪 Glycolic acid🡪 glycooxylic acid and oxalic acid
- Oxalic acid 🡪 combines with calcium to form calcium oxalate 🡪 hypocalcemia, QTc prolongation, renal stones
- Toxic effects
- CNS, Cardiopulmonary, Renal
- What do I see on labs?
- HAGMA
- Treatment- same as above
- Where can I find this?
11-11:30) Discharging the Intoxicated Patient – Holly Stankewicz, DO
- NEVER LET A DRUNK RUIN YOUR CAREER
- Clinically sober vs BAC🡪 Either way is fine as long as your documentation matches.
- I.E someone blows a very high BAC and one hour later you write “appears clinically sober” that doesn’t match
- If signs of trauma, EVALUATE closely.
- Make sure you are fully evaluating the intoxicated patient for signs of trauma/ need for further imaging.
- Make sure drunks are just drunk!
- Lots of pathology can look like intoxication.
- Be careful with AMA
- Pay close attention to vulnerable populations.
- All intoxicated minors should be discharged home with a parent not a sober friend
- Clinically sober vs BAC🡪 Either way is fine as long as your documentation matches.
11:30-12) Complications of Chronic Drug and Alcohol Abuse – Brian Kelly, DO
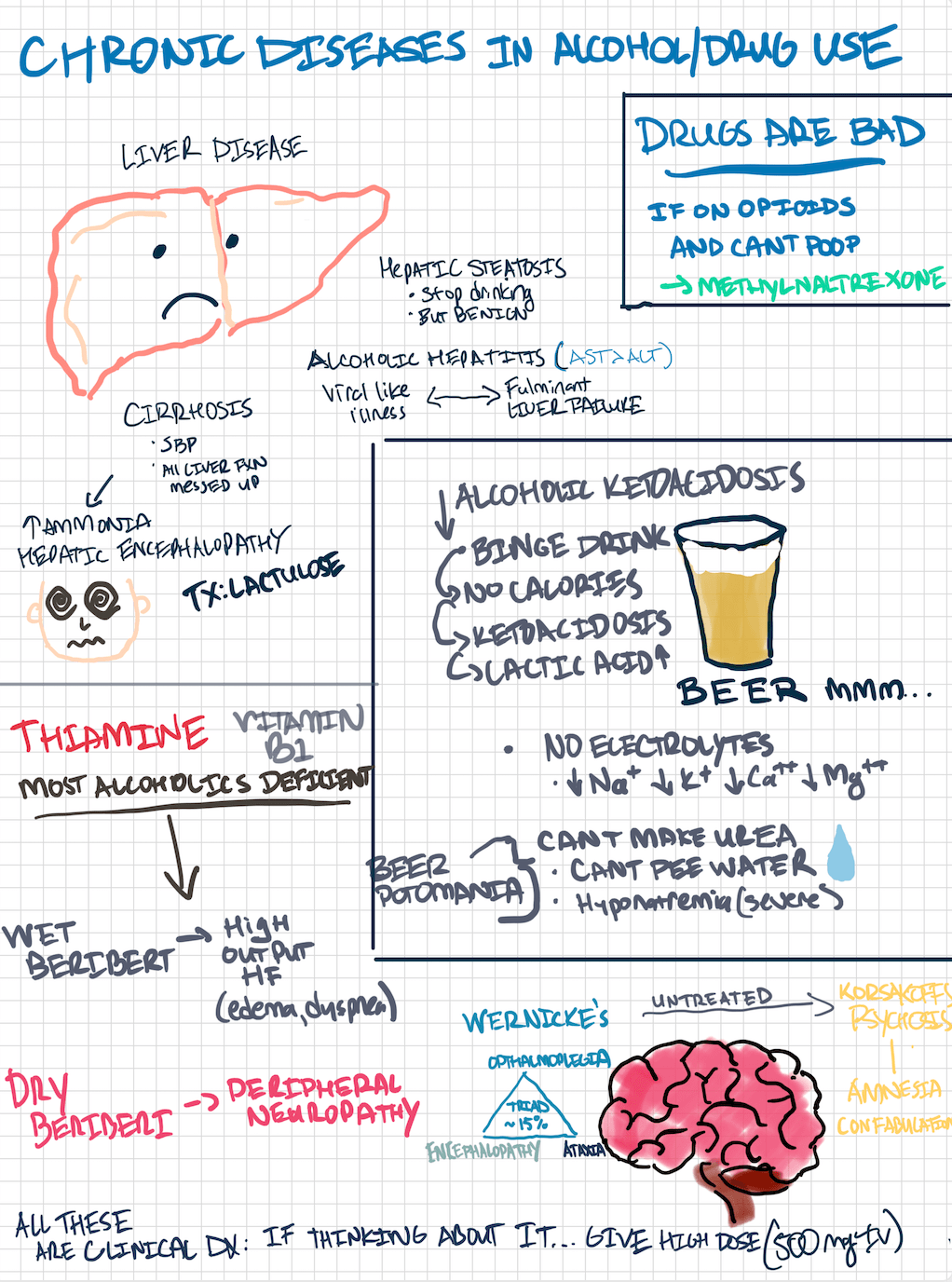
- Alcoholic Ketoacidosis
- Pathophysiology
- Ethanol metabolism depletes NAD stores
- Results in inhibition of Krebs cycle, depletion of glycogen stores, and ketone formation
- Suppresses gluconeogenesis and may result in hypoglycemia
- High NADH:NAD also results in increased lactate production
- Acetoacetate is metabolized to acetone so elevated osmolal gap may also be seen
- Ethanol metabolism depletes NAD stores
- Management:
- Thiamine prior to glucose to decrease risk of badness
- D5NS for hydration- dextrose treats the starvation ketosis aspect
- Oral nutrition if able
- Electrolyte replacement
- Pathophysiology
- Beer Potomania
- Electrolyte abnormalities that occur secondary to overconsumption of electrolyte poor liquid
- Hyponatremia, hypochloremia, hypokalemia
- Beriberi🡪 thiamine deficiency B1
- Dry: neuro symptoms
- Wet: cardiac symptoms
- Wernicke- Korsakoff syndrome–
- Wernicke encephalopathy
- Acute neurologic symptoms caused by thiamine deficiency
- werNICke
- Nystagmus/opthalmoplegia
- Incoordination/ataxia
- Confusion
- Korsakoff psychosis
- Chronic neurologica cute symptoms caused by the same
- Confabulations
- TX: high dose thiamine, replete electrolyte abnormalities, feed them
- Wernicke encephalopathy
12-12:30) EM Case Presentation – James White, MD (OPEN FRACTURE PT)
- Treat patients with open fractures as trauma patients, looking for concomitant life-threatening injuries as well as vascular injuries and compartment syndrome from the fracture.
- Can Consider using Gustilo-Anderson classification system in early consultation with orthopedics

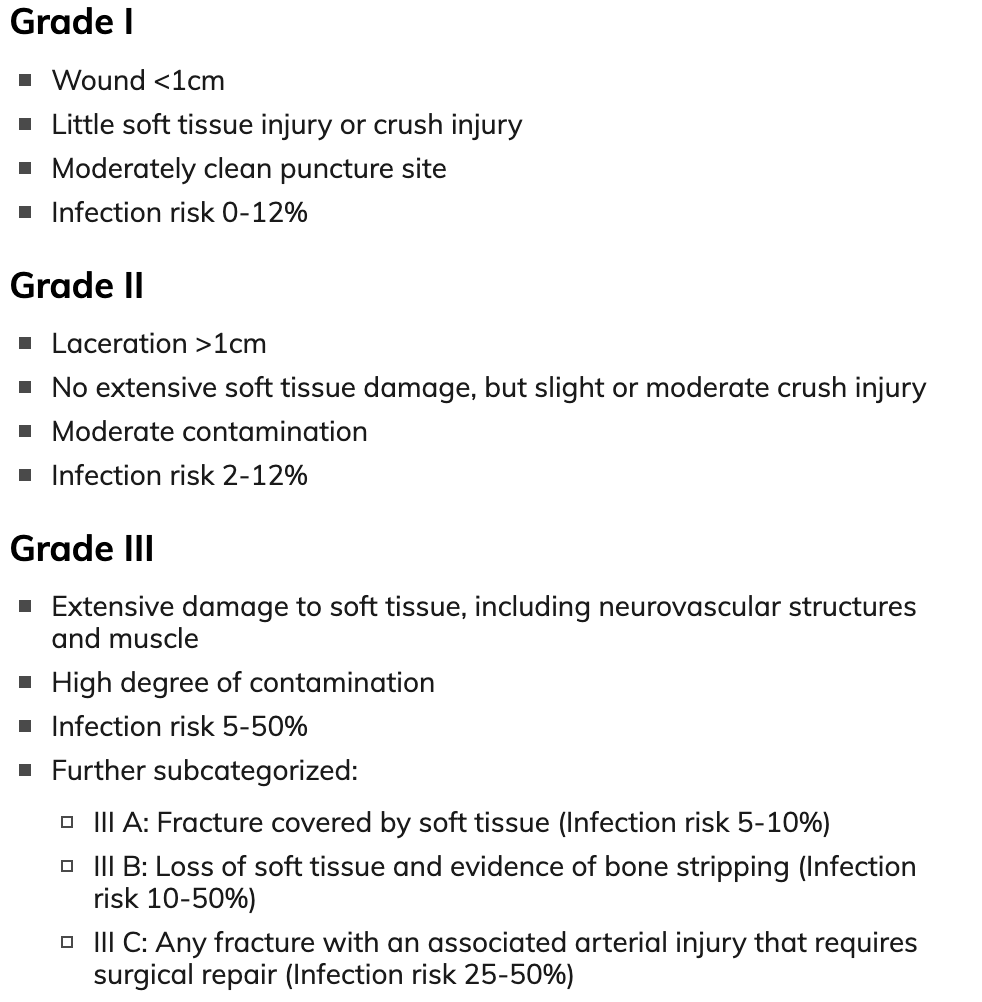
*as the grade increases so does risk of infection*
- Began early prophylactic antibiotics early with first-generation cephalosporin for Types I-II open fractures, and aminoglycoside or ceftriaxone to treat Type III
- Don’t forget Tetanus shots!
12:30-1) TRIAGE – chiefs
- TOXICOLOGY: Digoxin toxicity
- S&S: N/V/visual changes
- Mc visual change- yellow halos
- ECG: any dysrhythmia
- MC PVC
- ACUTE: bradycardia and heart block
- Chronic: ventricular dysrhythmias
- LABS: digoxin level, renal function, hyperK
- TX: digoxin specific antibody fragment
- Hypokalemia increases risk of digoxin toxicity
- S&S: N/V/visual changes
- Normal value for digoxin
- 0.5-2ng/mL
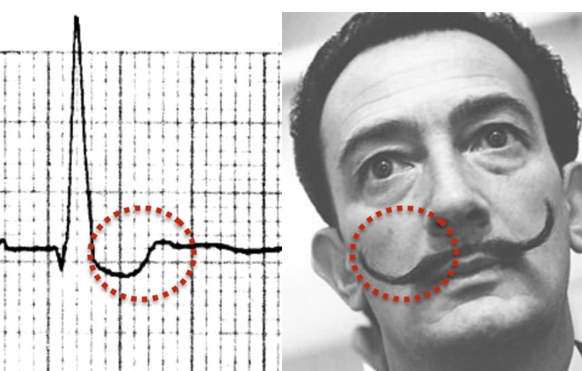
- Digoxin effect ECG
- Salvador Dali ECG sign
- Salvador Dali ECG sign
- RADIOLOGY: BENNET FRACTURE

- Fracture dislocation of base of metacarpal
- TX: Thumb spica and RICE
- INTEGUMENT: Sporotrichosis (Rose Gardeners disease)

- TX: itraconazole, fluconazole, amphotericin B (disseminated disease)
- ANCILLARY: Sign out culture



*** don’t leave dumpster fires***
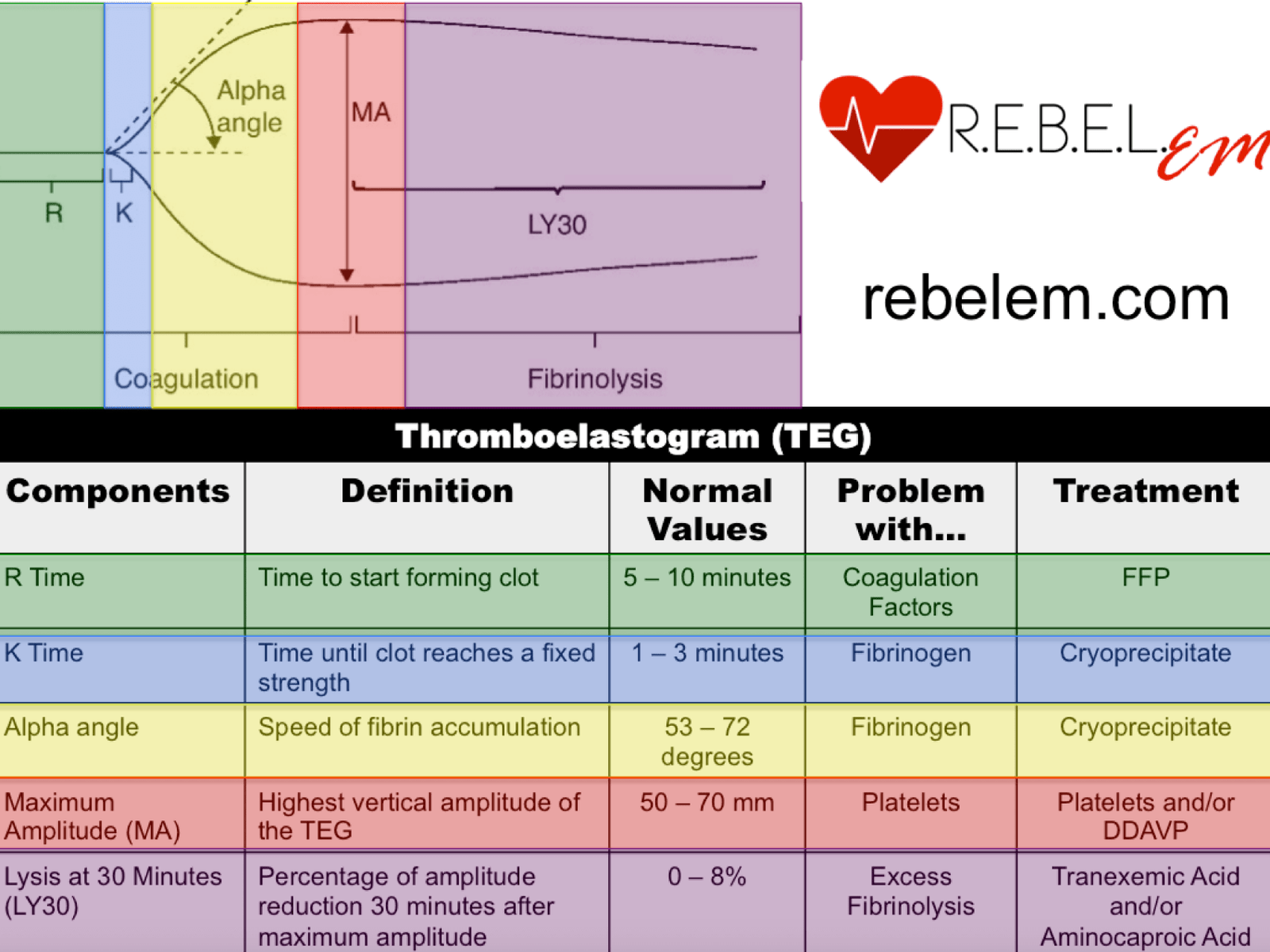
- GENERAL: TEG

- R (reaction time): time elapsed till clot initially forms.
- If the R time is elevated, this implies a deficiency in clotting factors. Replace them with fresh frozen plasma (FFP).
- K (K time): time elapsed till clot reaches a fixed strength of 20 mm.
- If elevated, fibrinogen is low. Replace with FFP/cryoprecipitate.
- Angle (clot kinetics): speed of fibrin accumulation.
- Low angle implies low fibrinogen. Replace with cryoprecipitate.
- MA (maximum amplitude): highest vertical amplitude.
- Low MA implies a qualitative or quantitative defect in platelets. Replace with platelets and/or DDAVP. A platelet function assay (PFA) may also be helpful to run.
- LY30 (lysis 30 minutes after MA): percentage of amplitude reduction 30 minutes after MA. Measures fibrinolysis.
- If high, treat with antifibrinolytics like aminocaproic acid or tranexamic acid (TXA).
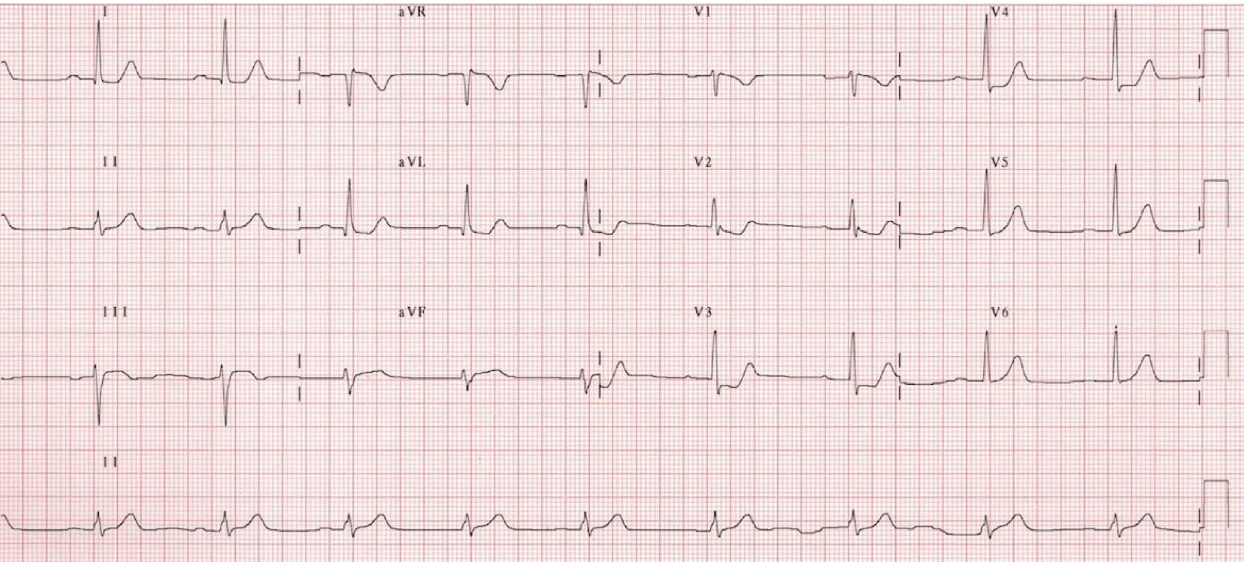
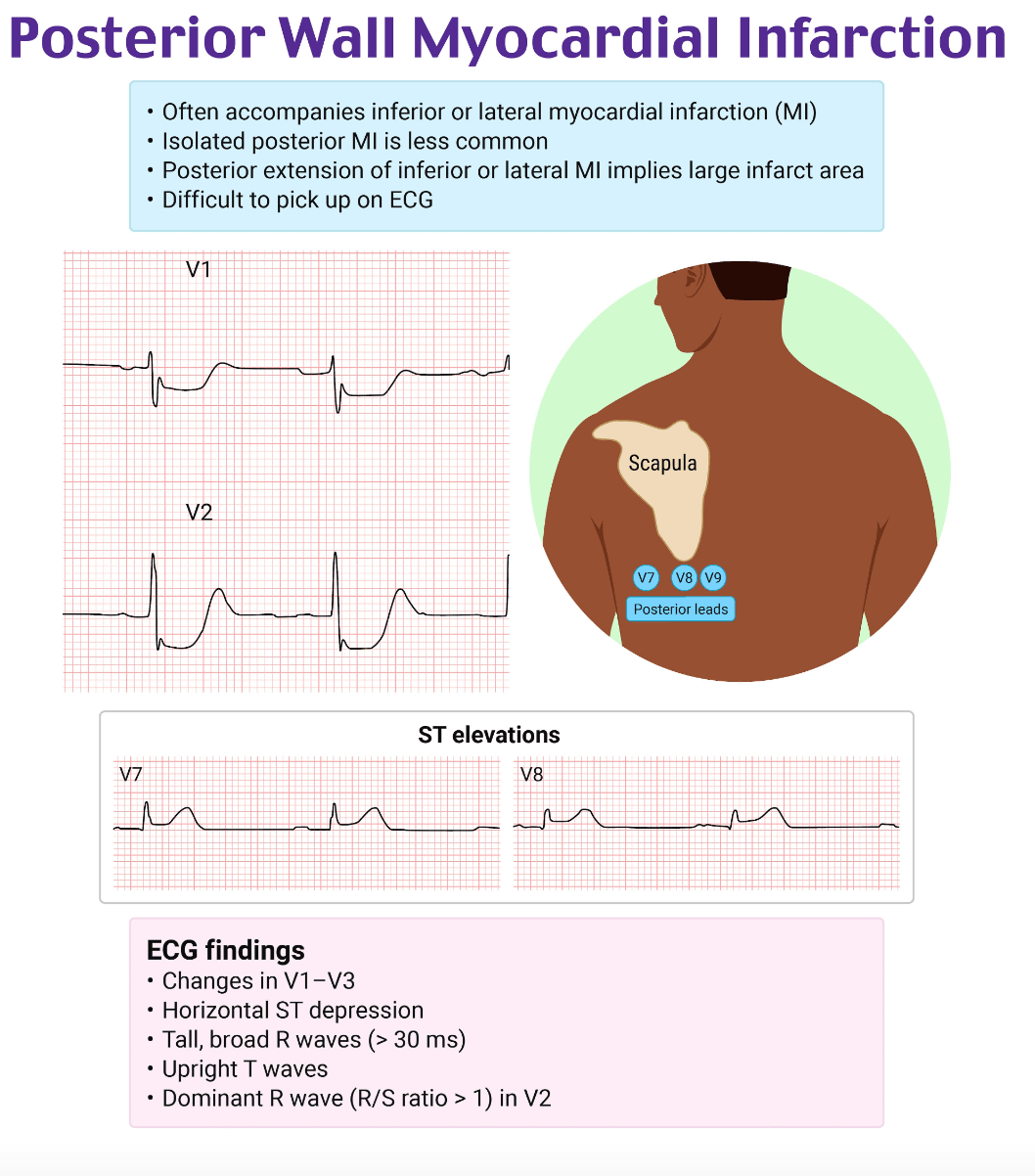
- EKG: Posterior MI