Syncope Patient: When to Worry & What to Do – Jonathan Pester, DO
- Syncope: brief loc + no tone + return to baseline
- Pathophysiology: 10 seconds of complete disruption 0f blood flow or nutrient delivery to both cerebral cortices or to the brainstem reticular activating system or reduction of cerebral perfusion by 35%
- IE. Inadeuate CPP
- Both Hemispheres of brain knocked out – RARE i.e stroke unlikely cause of syhncope
- RAS
- Sitting to standing
- Decrease venous return.
- Decrease cardiac output.
- Causes of syncope: THE LIST GOES ON AND ON
- Cardiac
- 6-month mortality >10%
- Structural problems of dysrhythmias
- Vasovagal and neurally or reflex medicated syncope- Most common
- Result of autonomic dysfunction
- SLOW PROGRESSIVE ONSET – PRODROME
- Orthostatic
- Postural hypotension – drop in sbp >20 or diastolic >10
- Psychiatric disorders
- Medications
- Neurologic disorders
- Isn’t syncope unless RETURNS TO BASELINE
- Cardiac
- Rule of 15s- 15% of the time these pathology presents with SYNCOPE
- SAH
- ACS
- Dissection
- PE
- Ruptured AAA
- Ruptured Ectopic
- CPP= MAP-ICP
- Syncope
- Prodrome
- No post ictal state
- Age >45
- Prolonged sitting/standing
- HX CHF- V important: biggest risk factor for mortality in SYNCOPE
- Seizure
- Prior hx
- Post ictal
- Age<45
- Event last ing >5 min
- Risk Stratification 🡪 USE YOUR BRAIN LOL
- San Francisco Syncope RULE- good things to keep in mind with syncope
- CHESS
- CHF
- Hct <30
- EKG abnormalities
- SBP <90
- SOB
- CHESS
- Boston Syncope RULE
- San Francisco Syncope RULE- good things to keep in mind with syncope
- SYNCOPE
- EVERYONE GETS AN EKG
- ORTHOSTATICS – Don’t mean anything you don’t have to do this just stand them up if they feel dizzy that’s enough.
- High Risk patients
- Abn ekg
- Decreased CO – HRxSR
- WOBBLER OR ABCDE,LR
- AV BLOCK
- BRUGADA
- QTc (Long or short)
- Delta – wpw
- Epsilong wave ARVC
- LVH/HCM
- Right heart strain
- Hct<30
- Abnormal EKG
- HEART FAILURE PATIENTS
- Abn ekg
Cardiovascular Complications In Pregnancy- Jason Becker, MD
- Lecture focusing on : After 20 weeks
- General stuff:
- 4 in 100 pregnant patients may experience a cardiovascular event during later pregnancy (2nd and 3rd trimester) or post-partum.
- Patients often lack traditional cardiac risk factors and may be unaware of any preexisting cardiovascular conditions at presentation.
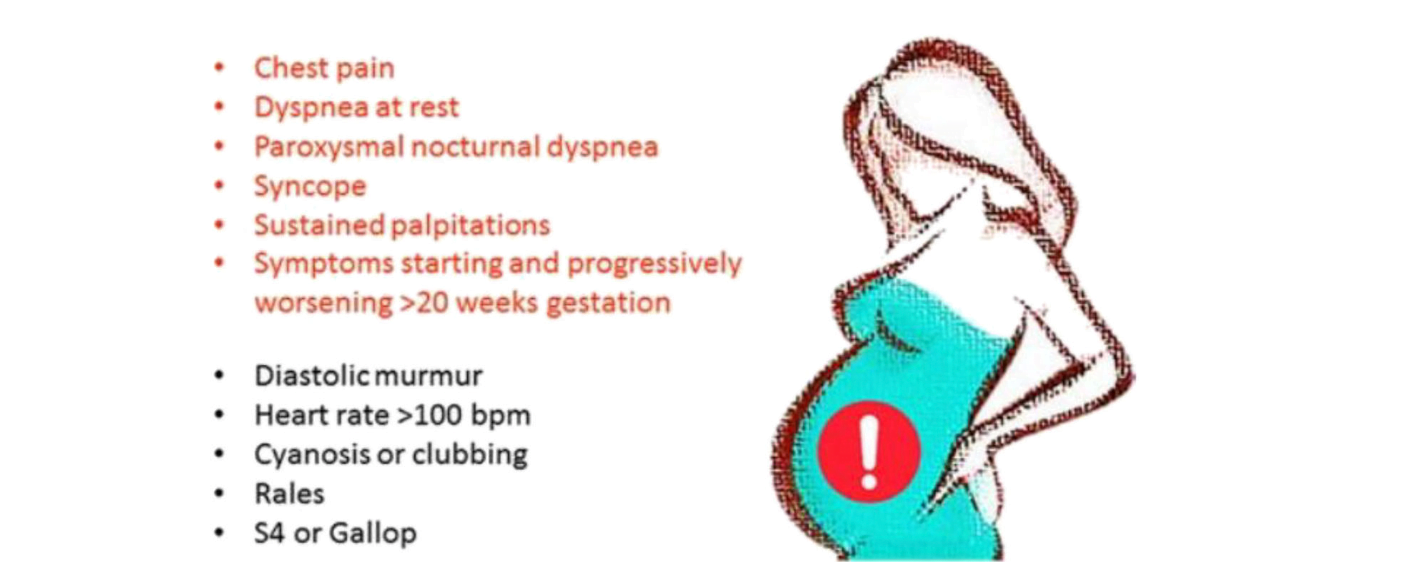
- “Red flag” symptoms and findings may include: chest pain, sustained palpitations, dyspnea at rest, unexplained tachycardia, syncope, findings of heart failure, or new murmur (diastolic or in context of new symptoms). Symptoms that begin after 20 weeks gestational age or progression of symptoms are concerning.
From: Lau E, O’Kelly A, Scott N. Pregnancy and cardiovascular disease. In: Aggarwal NR, Wood MJ, editors. Sex Differences in Cardiac Disease: Pathophysiology, Presentation, Diagnosis and Management. 1st ed. London: Elsevier; 2021. p. 390.
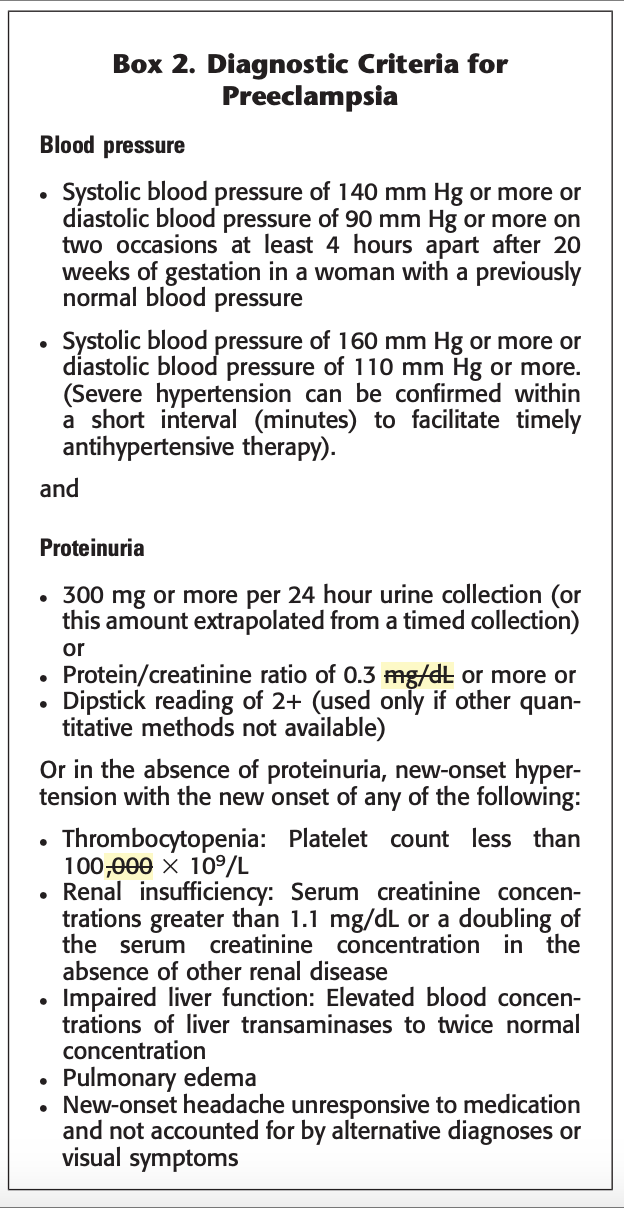
- Acquired hypertensive disorders of pregnancy
- Include: gestational hypertension, preeclampsia, eclampsia, and HELLP syndrome and are the 3rd leading cause of maternal and fetal morbidity and mortality in pregnancy per CDC.
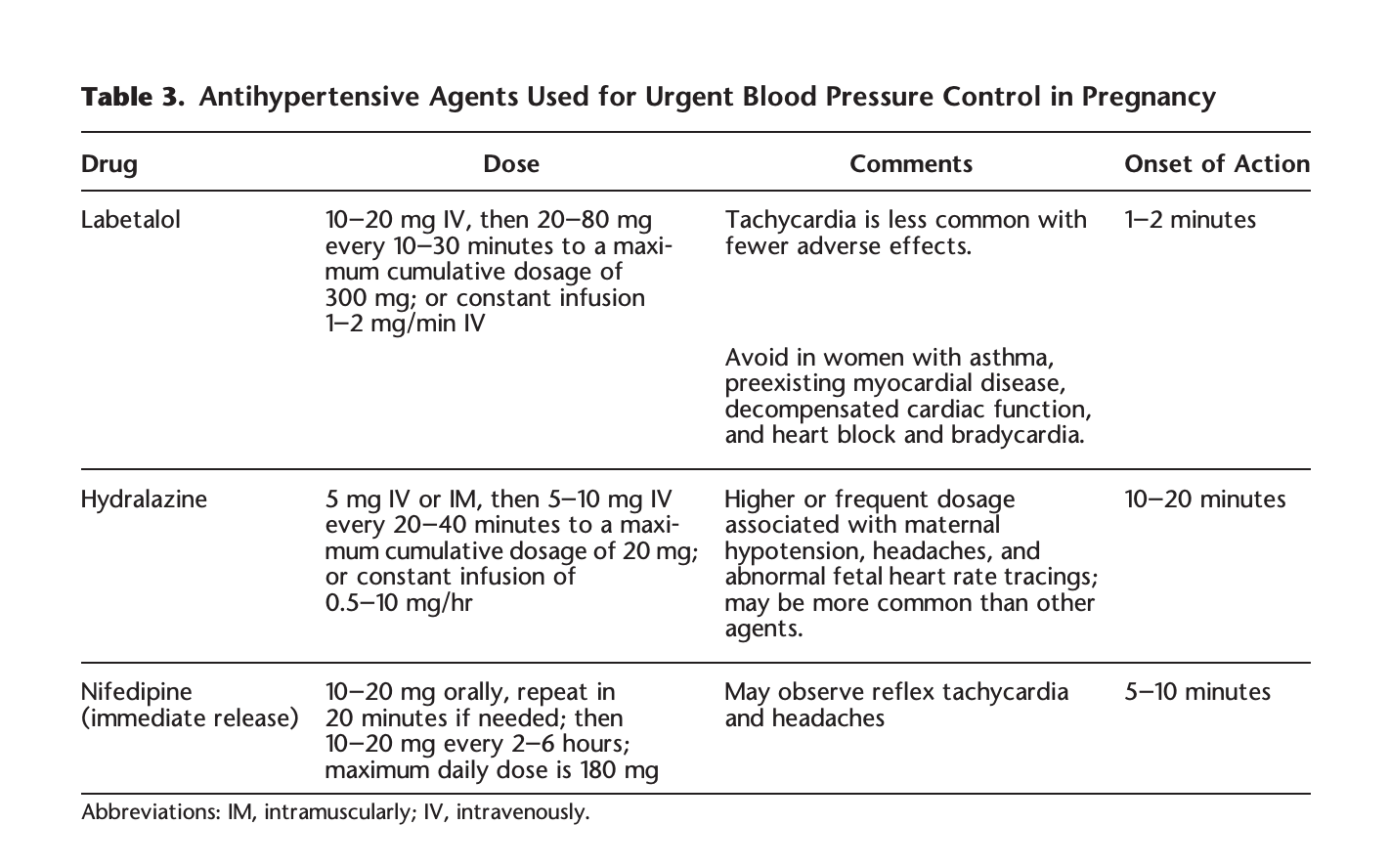
- Gestational hypertension is defined as BP > 140/90 measured on 2 occasions 4 hours apart in the absence of proteinuria or organ dysfunction at in a patient without prior history of hypertension after 20 wk gestation. Gestational HTN is defined as “severe” if BP > 160/110 X2 – usually measured minutes apart and IV BP management recommended in cases of severe gestational hypertension.
- Treatment of eclampsia and severe preeclampsia will require OB/GYN C/S, BP control and seizure prophylaxis (IV magnesium sulfate) for medical stabilization prior to delivery.
- Magnesium sulfate does require monitoring and frequent evaluation of patients for signs of magnesium toxicity (loss of DTR’s followed by apnea, and arrest). Rx: 10% calcium gluconate and Lasix, Intubation if indicated.
- Arrhythmias in Pregnancy
- Most common presentation associated with preexisting heart disease in pregnancy
- Pathologic: Superventricular Tachycardia(SVT)13%, Atrial fibrillation/flutter ( Afib/fl) 1.3%, Ventricular Tachycardia (VT) 1%, Cardiac Arrest (SCA) 4%
- DC cardioversion is indicated for all unstable tachydysrhythmias.
- Acute SVT 1st Line Vagal maneuvers and Adenosine. Preexcitation 1st line: Procainamide, or Flecanide with Beta blocker.
- Afib/Aflutter: Rate control 1st line Beta blockers with Anticoagulation (LMWH, UFH) preferred approach.
- VT: 1st Line Lidocaine, Procainamide and Beta blockers (Causes may include: CM, SCAD, MI)
- SCA: Per ACLS. Treat Aortocaval compression and Consider Resuscitative Hysterotomy in cardiac arrest.
Sumary Table:
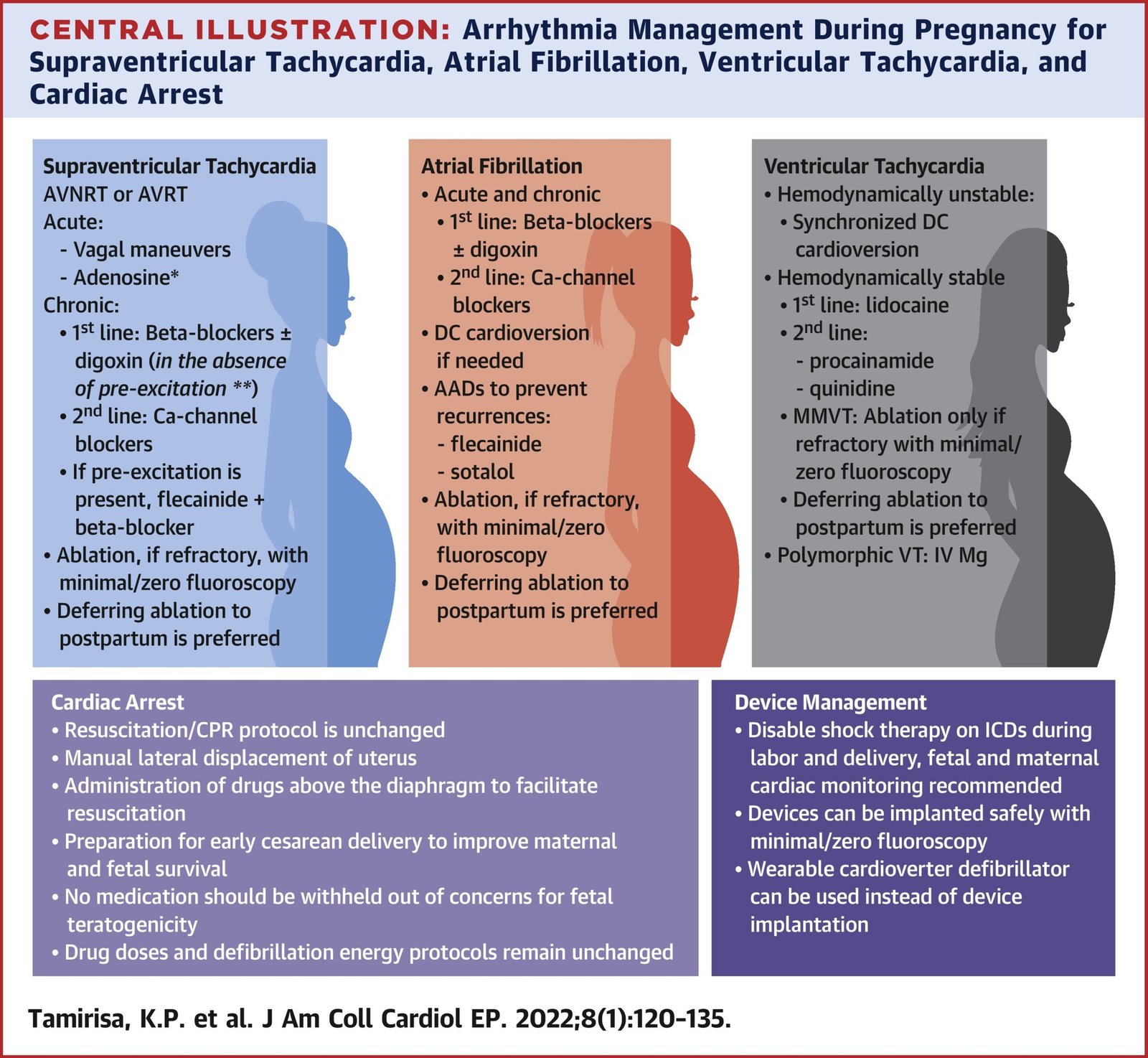
Link to above article: https://www.jacc.org/doi/10.1016/j.jacep.2021.10.004
- Cardiomyopathy in pregnancy:
- Top 3 causes of HF/Pregnancy: Peripartum CM (PPCM 68%), Dilated (DCM 6.9%) and Hypertophic (HCM 3.5%) (Data: Kaiser Permanente Study 2003-2014 patients presenting with HF in pregnancy)
- Preexisting CM may present with symptoms in 2nd trimester as maximal cardiovascular physiologic changes occur.
- PPCM: idiopathic HFrEF < 45%. Usually presents late in 3rd trimester and up to 5 months post- partum.
- Risk factors for PPCM include: Advanced age, African American Race, DM, HTN, Obesity and Preeclampsia.
- Initial Presentation PPCM may include: HF, Shock, Arrhythmias, SCA, CVA (Thromboembolic due to low EF).
- Up to 23% of HCM will present with HF or arrhythmia during pregnancy
- Rx: Optimize Preload (Volume Vs Diuretics SBP>110), Optimize HR and treat arrhythmias in HCM, Inotropes and possible mechanical support may be required in DCM/PPCM.
- Nitroglycerin, Lasix, Hydralazine, Beta blockade, Digoixin, UFH/LMWH may be used to treat HF in Pregnancy. Note: ACEI/ARB and Aldosterone antagonists are teratogenic and contraindicated in Pregnancy.
- Watch Volume/BP – Hypotension may worsen LVOT (HCM) and Placental Perfusion.
- Role of AC in CM with Low EF for stroke prevention.
https://www.ahajournals.org/doi/10.1161/CIRCHEARTFAILURE.120.008223
- Aortopathy in Pregnancy
- Majority of Aortic dissections in female patients under 35 years are associated with pregnancy or up to 12 weeks post partum.
- Majority will have preexisting condition: Bicuspid valve, Turner’s syndrome, Marfan’s, Ethlers-Danlos type IV as cause.
- Asymptomatic until they dissect – Patients may be unaware of preexisting aneurysm or hereditary condition until after event.
- Presentation in pregnancy may be typical (“chest pain +”) or atypical (e.g., limb ischemia, CVA, Abdominal pain).
- Dx: TEE, CTA or MRI without Gadolinium
- Rx: Type B – medical management
- RX: Type A – surgical repair may also include delivery by cesarian in in tandem – depending on GA and fetal viability
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5032923/
- Ischemic Heart Disease/Spontaneous Coronary Artery Dissection in Pregnancy:
- Rare in pregnancy but carries a 3 to 4-fold higher mortality than when present in non-pregnant patients.
- Causes AMI in pregnancy: Spontaneous coronary artery dissection (SCAD), Non-occlusive MI, Atherosclerosis.
- SCAD usually presents in late pregnancy early postpartum as STEMI, ventricular arrhythmia or SCA
- Diagnosis of SCAD at time of Cath.
- Rx SCAD: ASA and betablockade as PCI may worsen the dissection.
- Cath and PCI are indicated for all STEMI and Unstable NSTEMI in pregnancy.
www.jacc.org/doi/abs/10.1016/j.jacc.2020.05.084
TRIAGE- Dr. Garrett Jordan, DO
- Black widow vs. Brown Recluse
- Black widow- muscle cramping
- Brown recluse- local tissue destruction
- Pneumothorax ultrasound
- Sandy shore- normal
- Barcode- pneumothorax
- Hand foot and mouth
- Caused by coxsackie
- Self limited, supportive care
- Shoulder reduction
- Multiple options
- Cunningham technique is a simple first line option in a cooperative patient, and typically does not require any sedation
- Cardiac echo
- Views- parasternal long, parasternal short, apical, subcostal
- DeWinter
- STEMI equivalent
- LAD occlusion
July 20, 2023. Lecture Room 2
8) Acute Exacerbation of CHF – Jake Marais, MD
Reading: Chapter 53
https://www.emrap.org/episode/c3chf/c3chf
9) Childlife Specialist – Gretchen Duffy
9:30) Cardiology Cases – Multiple Faculty
10) Congenital Heart Disease – Rebecca Jeanmonod, MD
Reading: Chapter 129
10:30) Ventricular Tachyarrhythmias – Philip Salen, MD
11) Morbidity & Mortality Conference – David Pronchik, MD
12) EM Case Presentation – Dr. Seth Krivchenia
12:30) TRIAGE – Chiefs