Acute Heart Failure – Jake Marais, MD (For reference Chapter 53 Tintinalli)
- Basic definition of CHF: Functional impairment of ventricular filling or ejection of blood, leading to cardiac symptoms
- SOB, edema, fatigue, chest pain, exertional symptoms, weight gain, productive frothy cough, syncope
- Neurohormonal response to poor perfusion- catecholamine surge to compensate leading to sodium and water retention and increased systemic vascular resistance 🡪 worsen myocardial demand
- Goals of therapy:
- Reducing preload is an essential first step in overloaded patient
- Address afterload reduction – reduce Systemic vascular resistance
- Find the underlying causes – not necessarily in the ED
- Consider initiation of beta blockers if HD stable and without signs of low output – less important for ED presentation
- ** Acute heart failure management (what we do) – largely unchanged and mainly focuses on use of nitrates (preload reduction), diuretics, and positive pressure ventilation
- Cardiogenic shock in context of acute heart failure –
- weak pulses, tachy, cool extremities, JVD, hypoxia, hypotensive, narrow pulse pressure
- Why tachy? – compensatory
- Initiate Levophed and Milrinone immediately – Levo usually first, added Milrinone for peripheral perfusion later.
- Fluid challenge may be harmful in these patients due to cardiogenic shock component of their disease.
- Diuresis if/when hypotension improved/resolved
- Pulse pressure- difference between the systolic and diastolic pressures
- should be considered an additional vital sign especially in context of CHF.
- Generally, pulse pressures >40mmHg considered red flag
- If widened – think aortic insufficiency – backward flow across the aortic valve reduces the diastolic pressure and widens the gap.
- Poor perfusion in aortic insufficiency – massively reducing diastolic pressure – use nitroprusside, but very temporizing until aortic valve replacement
- HTN – #1 cause of heart failure – can be on boards
- Other risk factors – CAD, Age, diabetes, valvular heart disease, male sex, obesity
- One of the hallmarks in chronic decompensated CHF is diuretic therapy
- Often in the ED we underdose Lasix – onset of action 25-90 minutes
- In Lasix naïve patient – reach for 40 IV
- In patient on chronic diuretic therapy – can reach for 80-100 mg IV or use 2.5x the home dose in IV form
- i.e. 40 PO BID home furosemide = 80-100 mg IV
- Noninvasive ventilation
- BiPAP or high flow nasal cannula
- Reduces need for intubation, effect on mortality remains undetermined
- Improves ventilation by opening alveoli, fluid suppression, and dead space ventilation
- Requires close monitoring, proper facial anatomy, proper sea
- Don’t use Cardizem or Verapemil in acute CHF
- Negative inotropic action can worsen heart failure
- If Afib and heart failure, consider Digoxin – get rate control without negative inotrope
Shocking Arrhythmias – Dr. Salen (For reference Chapter 18 Tintinalli)
- Criteria for diagnosis of Wide complex tachycardia?
- QRS >120ms
- HR >100 for an adult
- Causes of wide complex – A LOT
- Illness
- Medication effect (sodium channel blockade)
- Bundle branch blocks
- Hyperkalemia
- Ventricular preexcitation syndrome
- Ischemic heart disease/MI
- Dilated hypertrophic cardiomyopathy
- Inherited ion channel abnormalities
- 4 EKG issues to consider whenever looking WCT
- Is it truly tachycardic?
- How wide is it?
- Is it regular/irregular?
- Do QRS complexes look the same or different?
- Do Wide complex tachycardias originate above or below the AV node?
- Can be both
- Supraventricular tachychardia with aberrant conduction such as a bundle branch block
- V-tach
- Can be both
- What is the difference between sustained and nonsustaned VT?
- V-Tach – occurrence of 3 or more consecutive PVCs
- Sustained – more than 30 PVCs in a row
- Why is VT bad? – rate is so fast that the LV can’t fill, lose the atrial kick which is responsible for 10-20% of LVEF
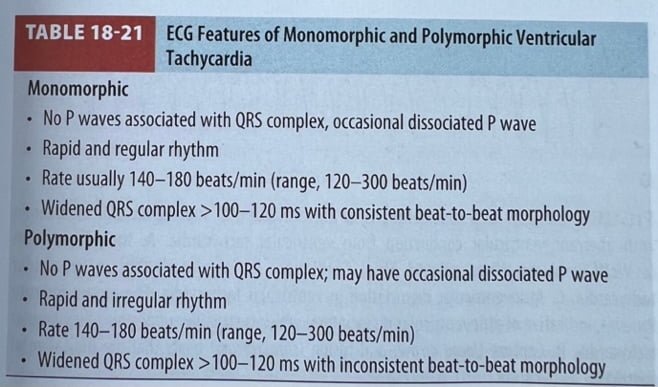
 Different Types of VT?
Different Types of VT?- Monomorphic (70%), Polymorphic (Torsades)
- Would like to know if they have a pulse with either – stable vs. unstable. But polymorphic VT is inherently very unstable to begin with.
- Stable 🡪 try rhythm control with meds
- Unstable 🡪 Cardioversion
- What are options for sustained, refractory monomorphic VT?
- Amiodarone -150 mg with pulse
- Amiodarone – 300 mg without pulse
- Lidocaine also an option
- Procainamide also option – but proarrhythmic, makes you hypotensive
- Cardioversion (unstable patient) – try to administer Amiodarone before cardioversion, makes it more successful according to multiple studies
- Polymorphic VT
- Torsades – has long QT – give Mg Iv
- Potentially degenerates into V-fib arrest
- Long QT syndrome – beta blockers to slow the HR, get AICD
 Different Types of VT?
Different Types of VT?Further reading: https://litfl.com/ventricular-tachycardia-monomorphic-ecg-library/
Congenital Heart Disease – RJ (For reference Chapter 129 Tintinalli)
- The Sick Baby
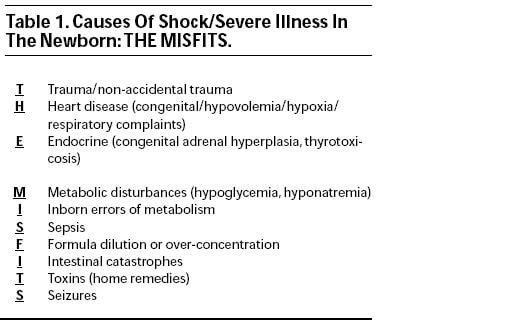
- THE MISFITS
- Have a mantra for panic: “Air goes in and out, blood goes round and round. And that’s really it.”
- Review Fetal Circulation
- Fetal circulation bypasses the lungs cuz they don’t work….yet
- Oxygenated blood from umbilical vein to the fetus
- Umbilical vein 🡪 Ductus venosus 🡪 IVC
- R heart 🡪 Ductus arteriosus or the foramen ovale 🡪 L heart 🡪 systemic circulation
- In utero, R sided circulation predominates
- Changes at birth
- When newborn takes first breath, everything changes
- Pulmonary vascular resistance falls as lungs fill with air
- Rush of blood from the RV to the lungs
- Blood returns from lungs to the L heart, increasing L heart pressure which subsequently closes foramen ovale to minimize shunting
- Decreased prostaglandin synthesis at birth (due to loss of placenta) and the ductus arteriosus starts to close
- Because neonates have noncompliant ventricular walls, they can’t really change stroke volume in response to stress, so they will change HR in response to stress 🡪 sinus tachycardia
- Ductus arteriosus – closed by 15 hours of life
- Foramen ovale – closed by 3 months of life
- Blue Babies – mixing of deoxygenated and oxygenated blood or R to L shunting
- Tetralogy
- Transposition
- Truncus arteriosus
- Tricuspid atresia
- Total anomalous pulmonary venous return
- Pink babies – pulmonary overload
- VSD
- ASD
- PDA
- Coarctation
- Many of these lesions you will be unable to fix – your job is to stabilize
Further reading:
https://emergencymedicinecases.com/video/congenital-heart-disease-emergencies-p1/
https://emergencymedicinecases.com/video/congenital-heart-disease-p2/
Childlife Specialist – Gretchen Duffy
- Child life specialists are there to help with difficult children and their families
- Can help occupy the child during procedures, have suggestions for pain control, positioning for procedures
- Place consult to child life in epic – should pop up
- 7a-3pm for now
Triage – Dan Greco
- Jellyfish stings
- Don’t pee on it
- Step 1: Salt water immersion
- Step 2: Vinegar
- Step 3: Hot water immersion
- ** If Portuguese man of war – vinegar probs won’t help
- Fishhook removal: https://www.youtube.com/watch?v=-2Re91_P7KE
- Herpetic Whitlow
- Viral infection caused by hsv1 or hsv2
 Direct digital contact with secretions from lesions of infected
Direct digital contact with secretions from lesions of infected- Localized burning, itching, pain preceding classic herpetic vesicles
- Usually affects 1 digit
- Abx and drainage not necessary
- Contagious until lesions crusted
- Can last 2-3 weeks
- Tx:
- Primary – anti-inflammatories and/or topical acyclovir (?)
- Recurrent/multiple sites/immunocompromised – Oral/iv acyclovir
 Direct digital contact with secretions from lesions of infected
Direct digital contact with secretions from lesions of infected