November 2, 2023
DKA and Hyperosmolar states- Philip Salen, MD
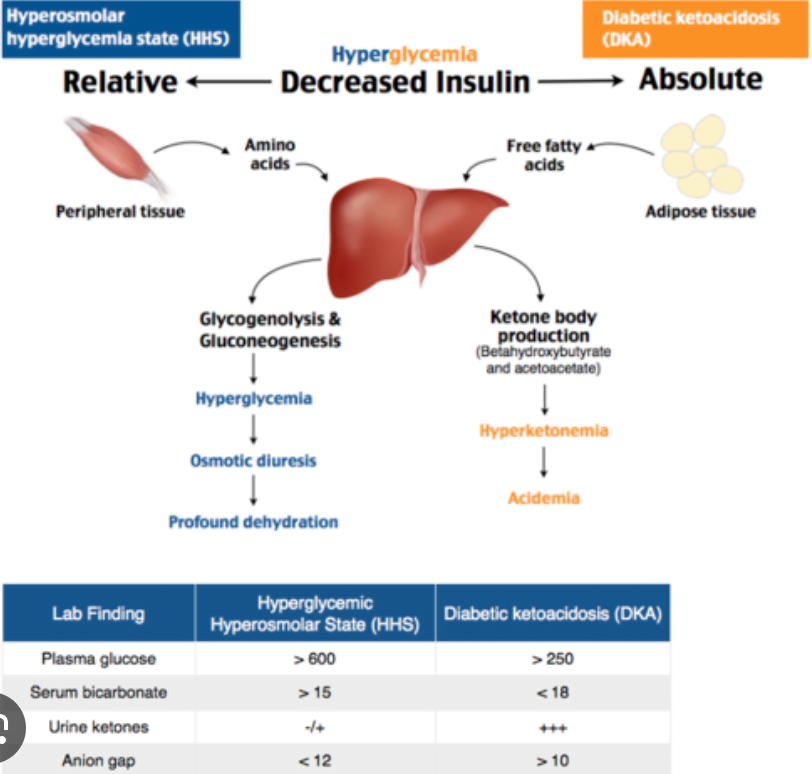
DKA – no insulin — lipolysis — ketone
Imp labs – CBC, CMP, lactate, VBG, UA, Beta hydroxybutyrate.
Treatment Goals f or DKA – close the GAP, fluids, Insulin + Dextrose, treat hypokalemia.
Best crystalloid : NSS or buffered “balanced” crystalloids.
Treatment complications – cerebral edema: probably secondary to administering of Bicarb. AVOID Bicarb. Severity of illness also predisposes to cerebral edema. Get CT scan.
Insulin trip, after taking care of the K. 0.1unit/kg insulin bolus. 0.1 u/kg/hr.
If they have an insulin pump, hold it.
If glucose is < 250 add dextrose to IVF.
DON’T give insulin if they are hypokalemic ( follow the algorithm)
Dispo : ICU vs floor ( mild DKA)
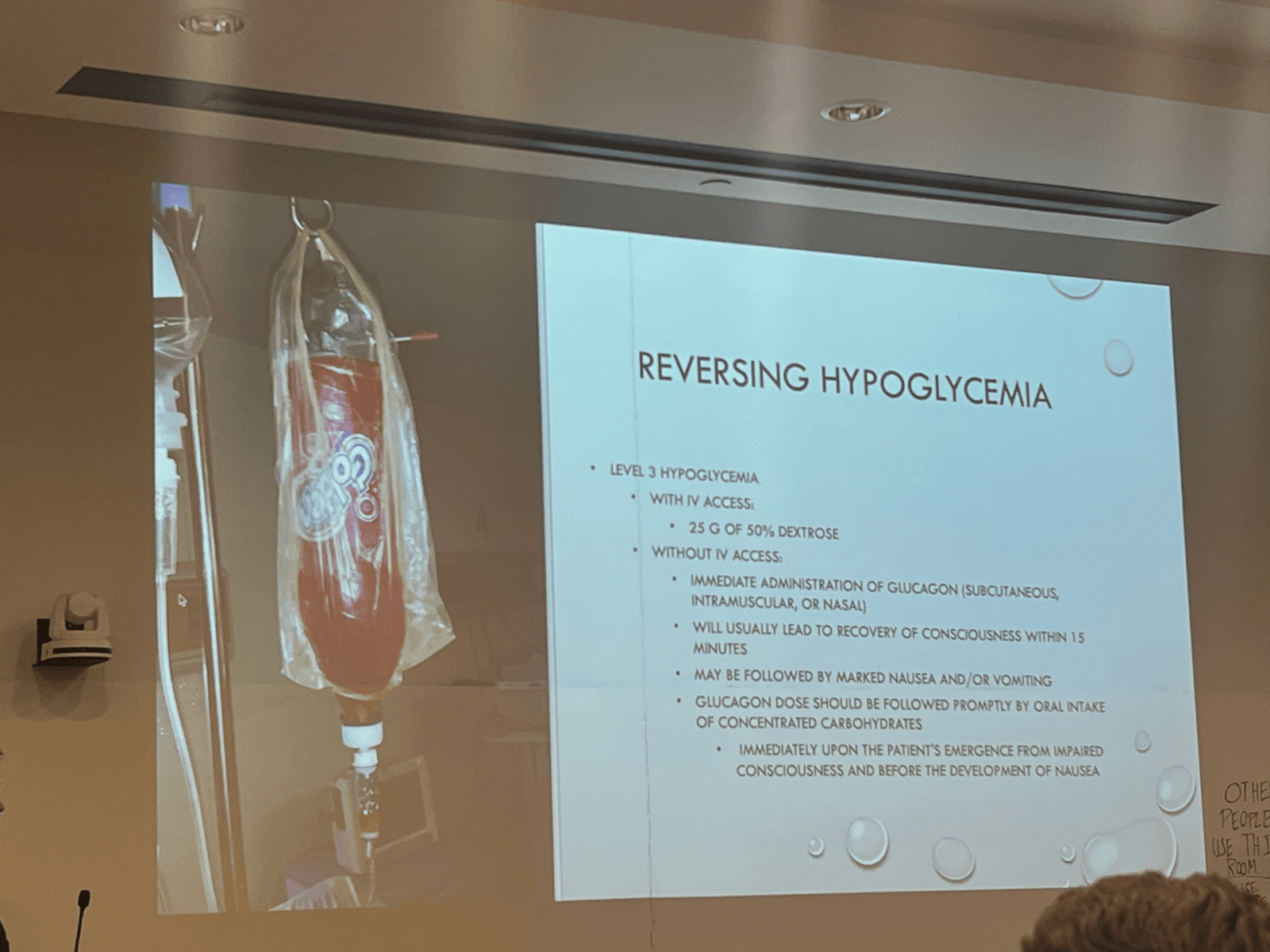
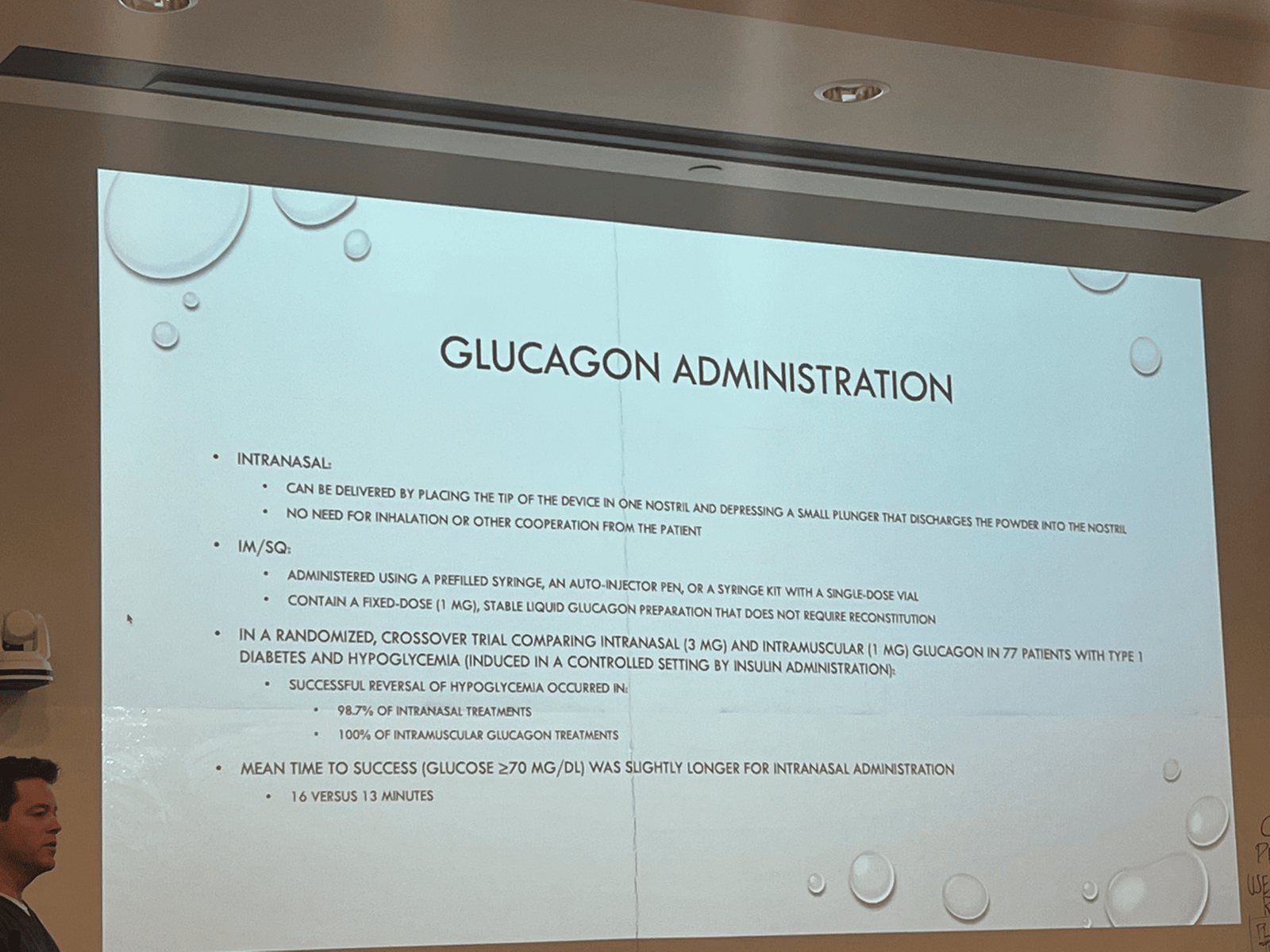
Hypoglycemia treatment : glucose, glucagon, Octreotide ( if on sulphonylureas)
HHS :
Therapy same as HHS, but slowly.
Hypoglycemia- Patrick Cheatle, MD
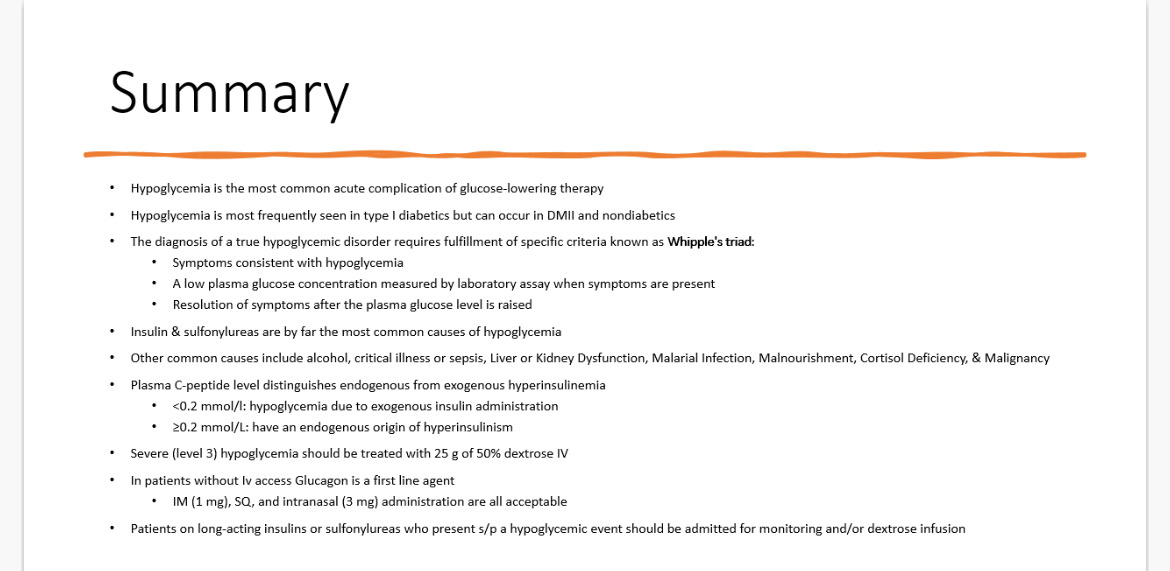
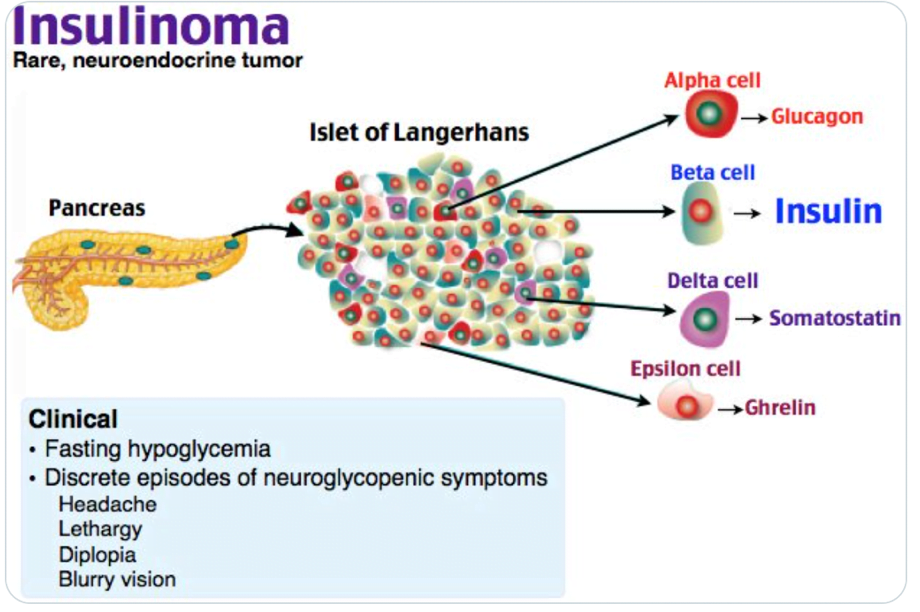
Whipple triad
Symptoms consistent with hypoglycemia
A low plasma glucose conc measured by laboratory assay when symptoms are presents
Resolution of symptoms when sugar is normalized.
Clinical manifestation – non specific, autonomic and neuroglycopenic symptoms.
Causes of hypoglycemia –
Drugs : insulin, sulfonylureas, quinolones, beta blockers, ACE-I, insulin like growth factor.
Alcohol – ethanol inhibits gluconeogenesis.
Critical illness, sepsis. Cytokine mediated. Uptakes glucose utilization.
Liver kidney dysfunction
Cortisol deficiency
Malarial infection AND treatment
Malignancy.
Malnutrition.
Endogenous Hyperinsulinism – insulin secretion fails to fall appropriately in the setting of hypoglycemia.
Accidental, surreptitious or malicious hypoglycemia – accidental ingestion, herbal products, exogenous ingestion
Jamaican Vomiting Illness : Ackee fruit , if you eat raw form it – causes severe hypoglycemia.
If you have a reason for hypoglycemia – treat
If unknown cause, more work up
C-peptide : distinguishes endogenous from exogenous hyperinsulinemia.
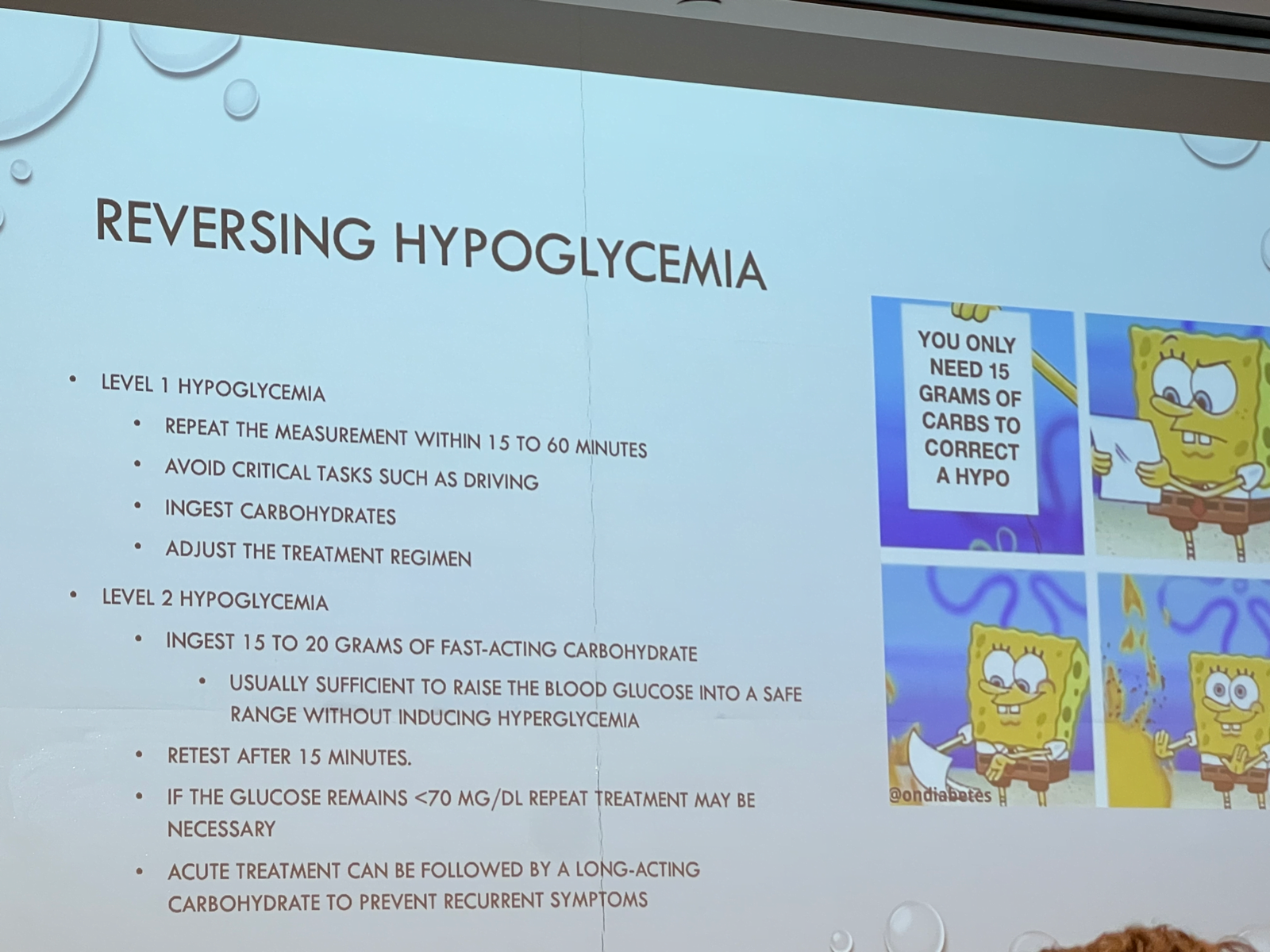
Classification
Level 1: 54 to 70
Level 2: < 54
Level 3 hypoglycemia event that required the assistance of another person to actively administer carbohydrate, glucagon, or other resuscitative action.
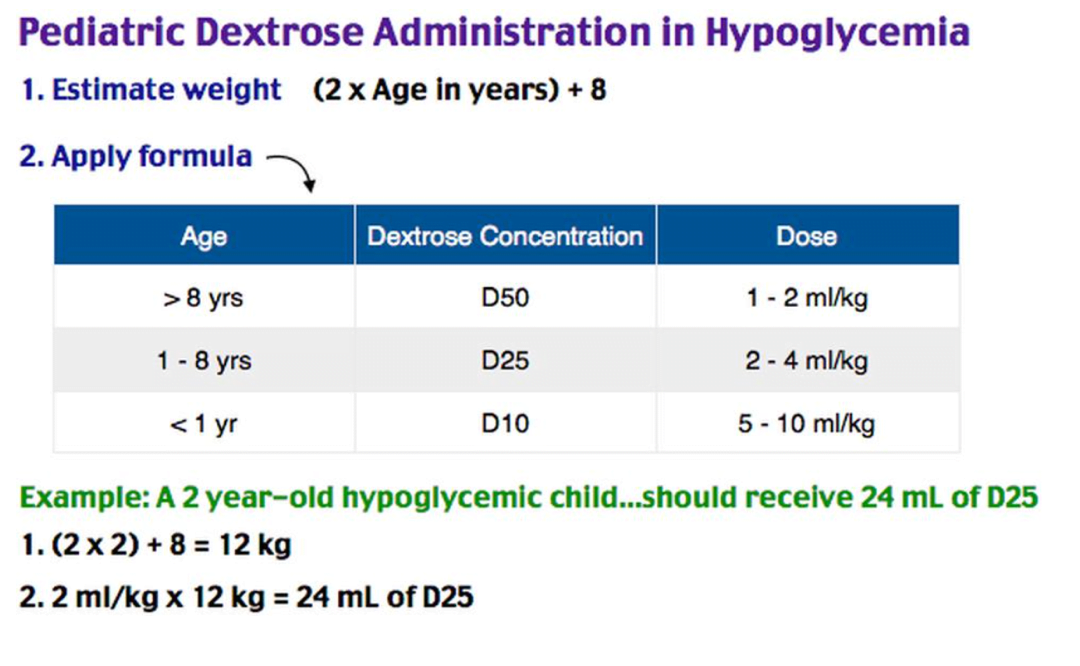
Treatment:
Monitoring: glycemic response if transient. Might need infusion, or observe + po intake.
Repeat blood sugar.
Diseases of Adrenal Gland – Brian Kelly, DO
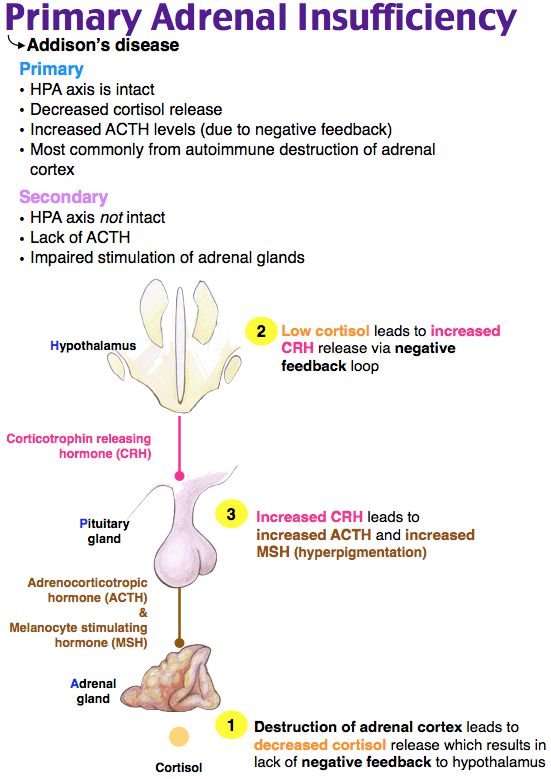
Hypothalamus – CRH – Anterior Pituitary – ACTC – Adrenal glands – cortisol, androgens aldosterone.
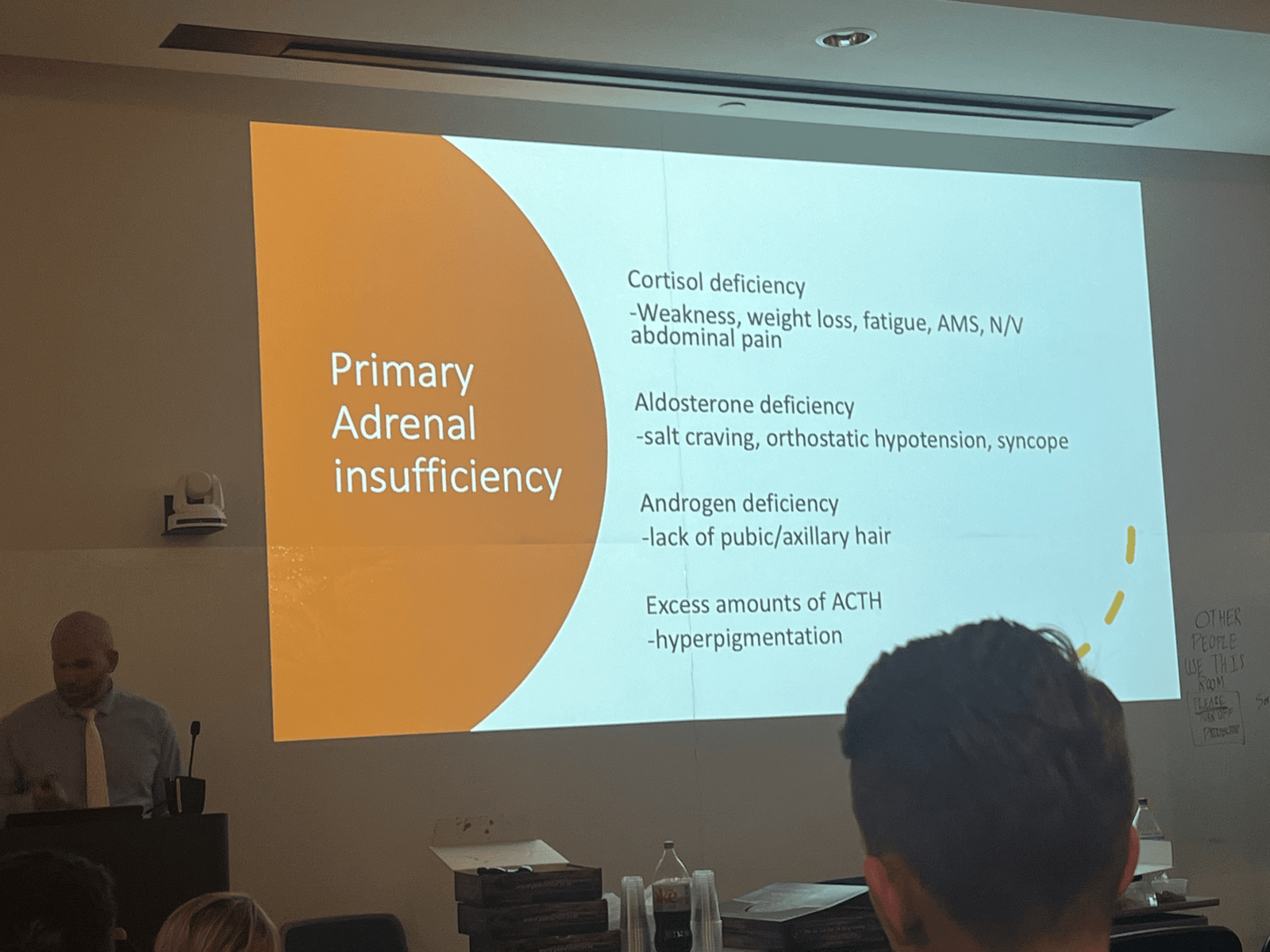
Addison’s disease , primary adrenal insufficiency
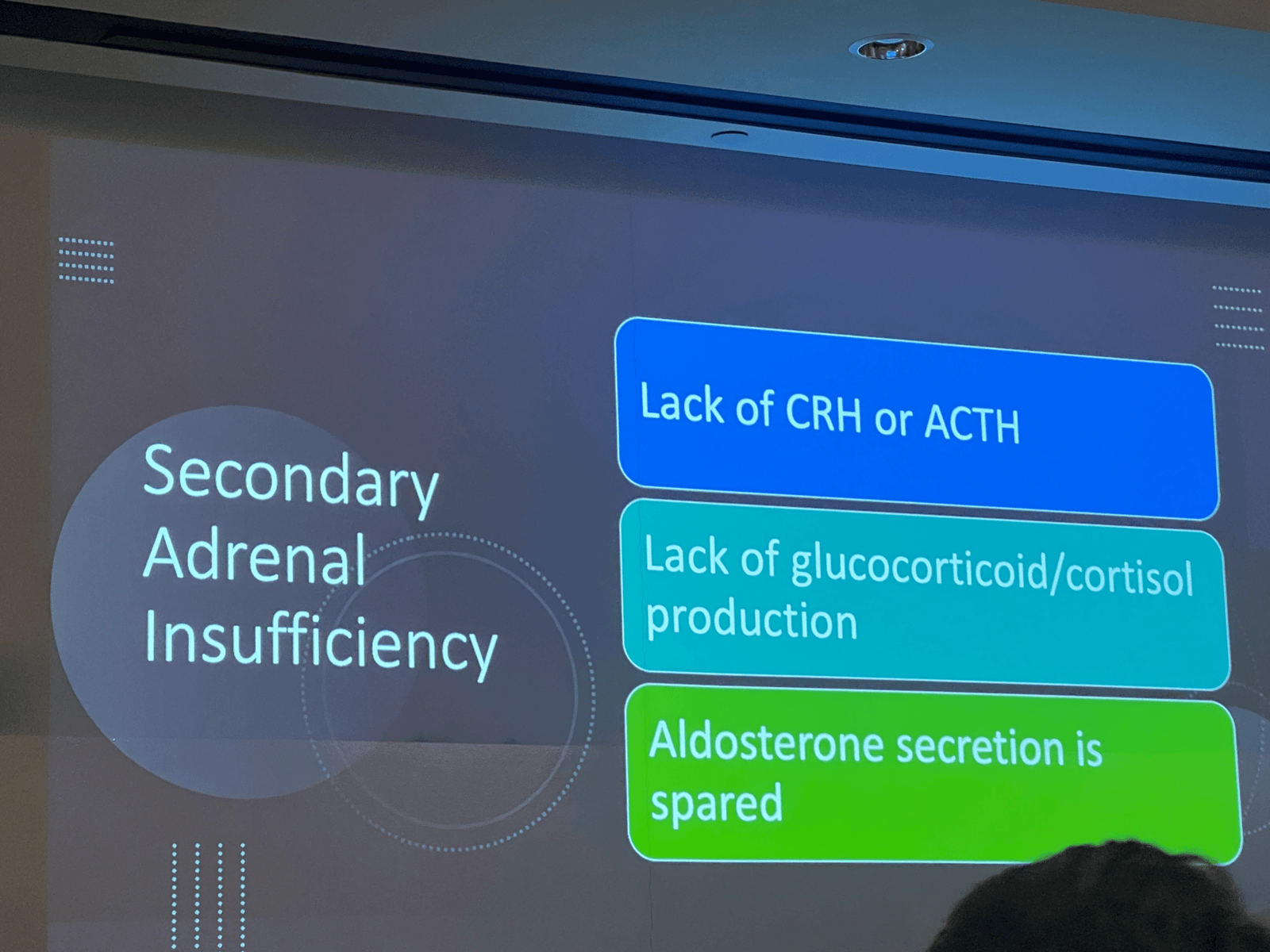
Secondary Adrenal Insufficiency :
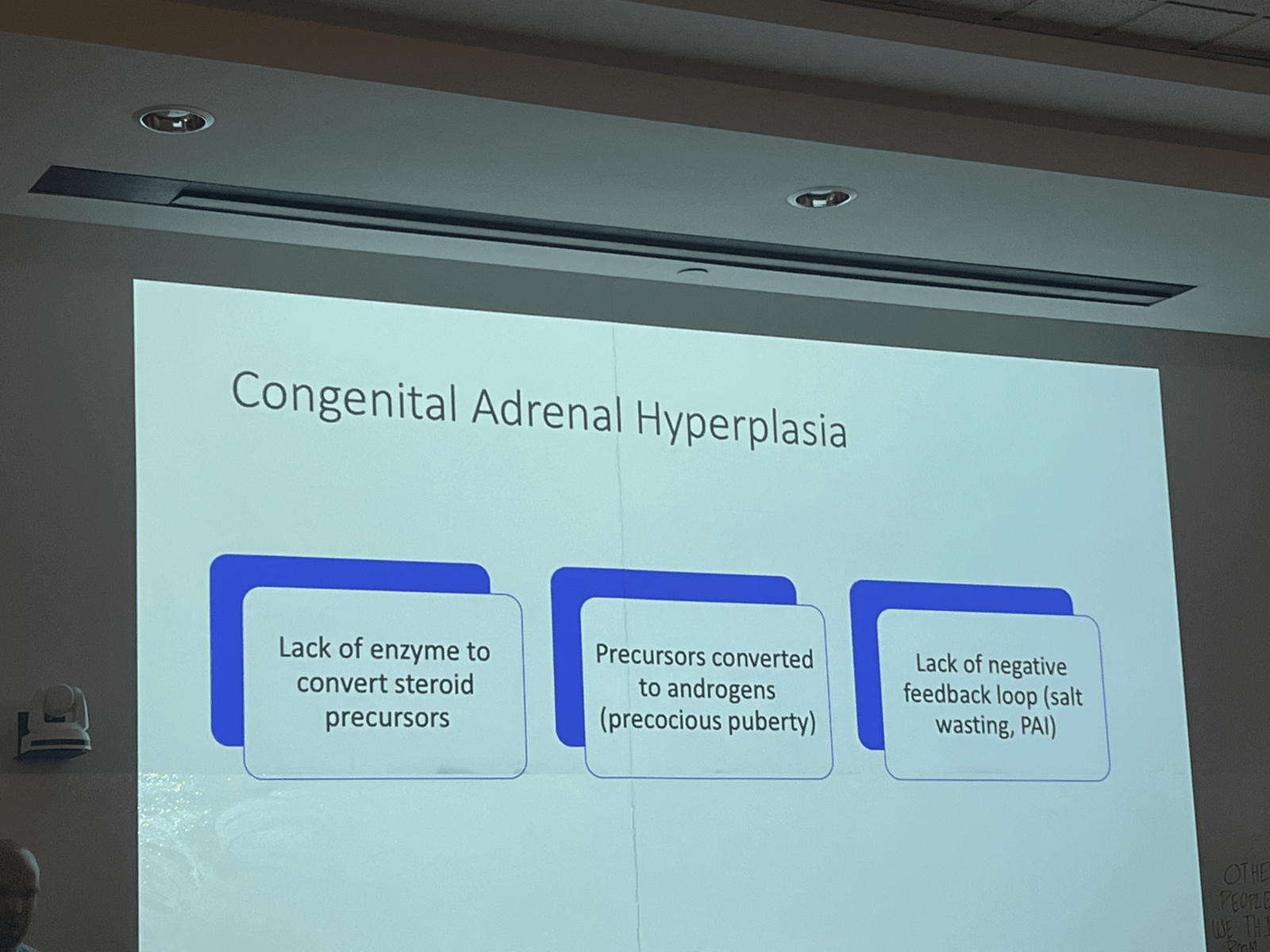
Congenital Adrenal Hyperplasia
Adrenal Crisis
- Hypotension
- NV
- Fatigue
- Fever
- Somolence
- Hyponatremia/hyperkalemia/hypoglycemia
PMH: Addison, Adrenal diseases, TBI, Steroid use, Autoimmune disease
Precipitating factors : recent med changes, recent surgery, major trauma, pregnancy
PE : AMS, Dry MM< Hyperpigmentation, Hypotension, Alopecia, Abd tenderness, tachycardia.
Seem sicker than they should be, persistent hypotension, Greater than expected AMS, new hyperkalemia with hyponatremia hypoglycemia, refractory hypotension in septic shock.
Testing : Basic lytes, Random cortisol not very helpful, ACTC stim test ( ICU),
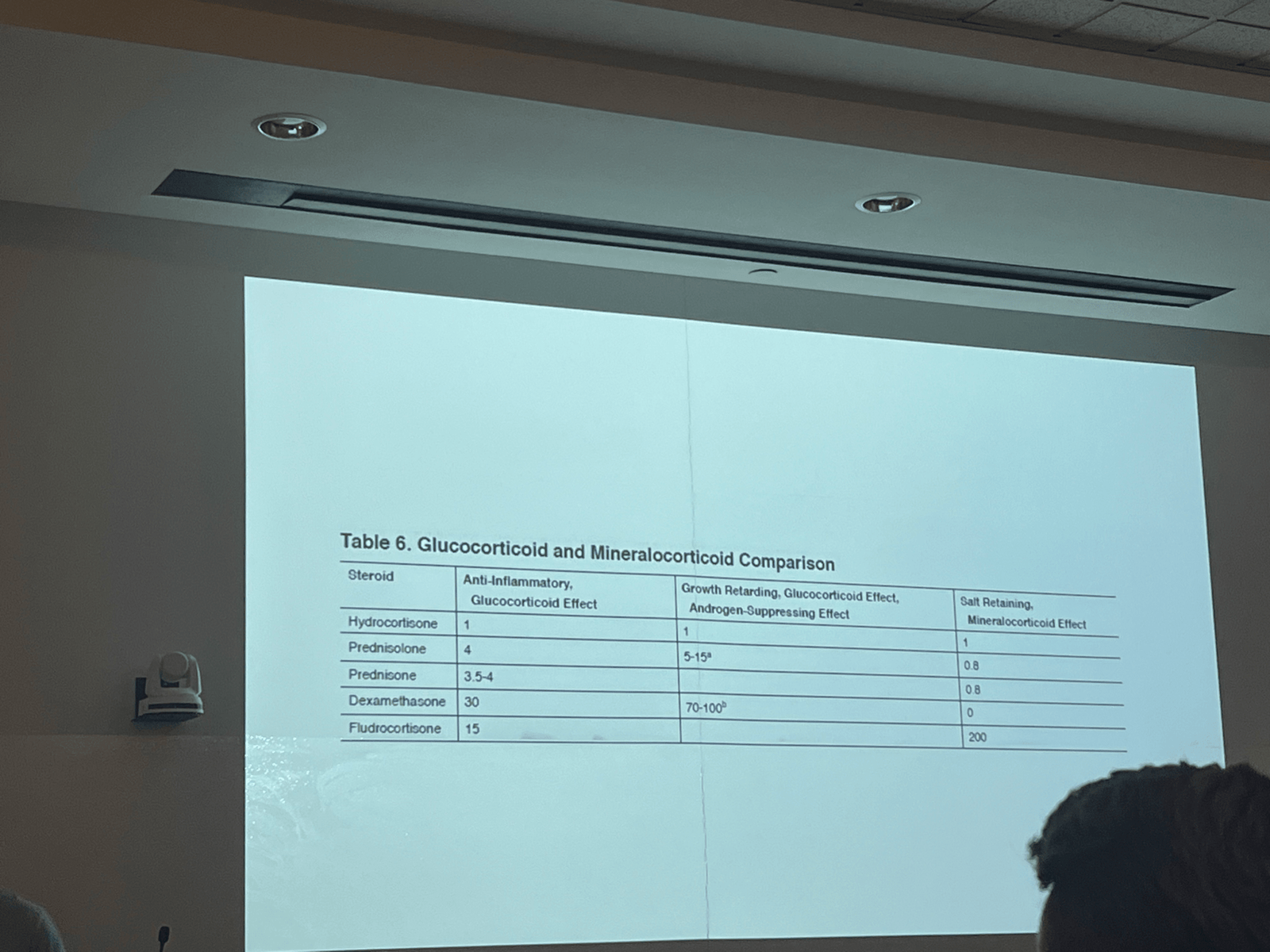
Treatment :: Stress dose steroids. Hydrocortisone 100 mg IV, 50 mg kids, 25 mg neonates.
CITCI – Critical Illness Related Corticosteroid Insufficiency.
Sepsis and Cardiac Arrest – should we give steroids? No significant data.
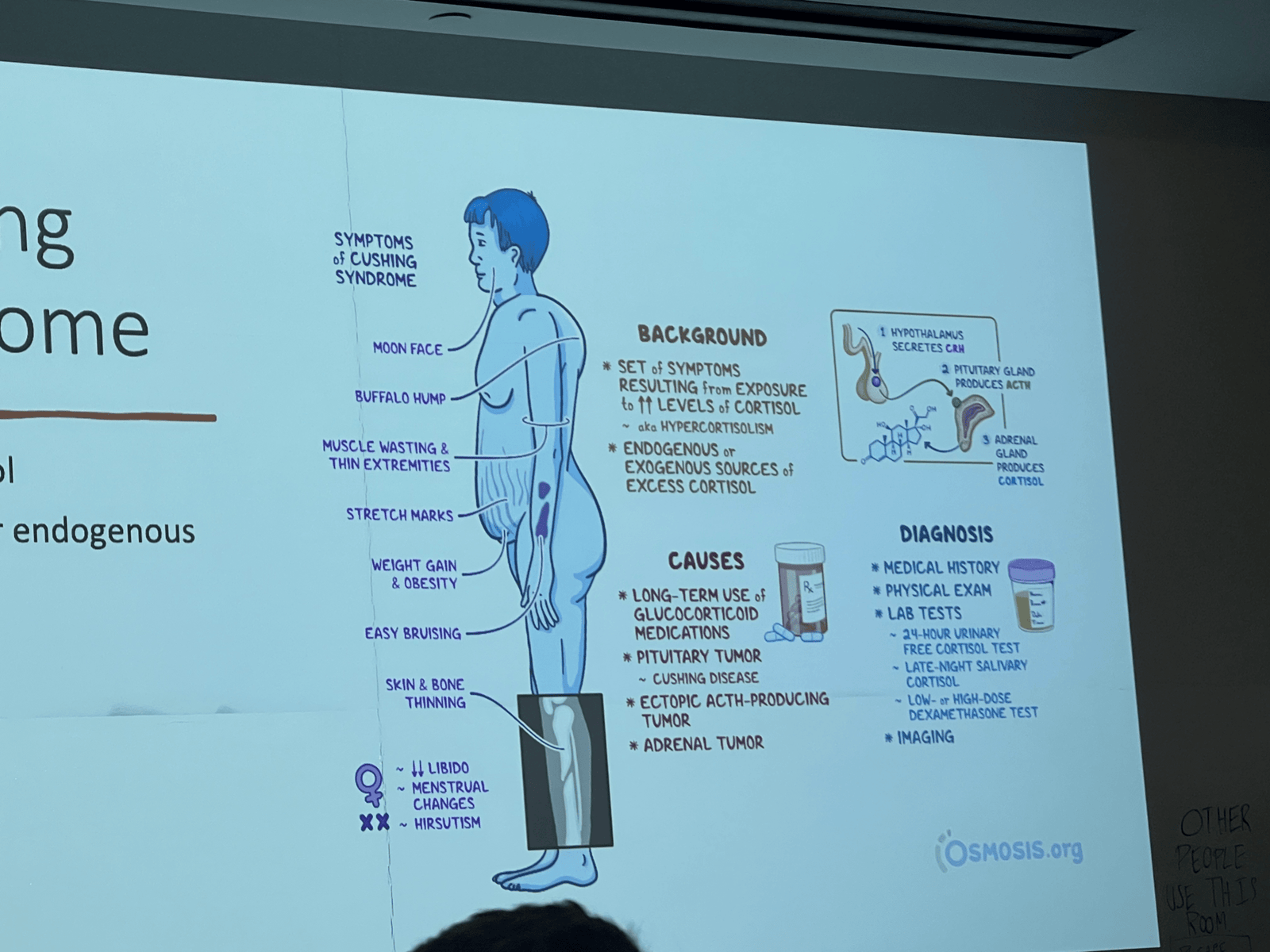
Cushing Syndrome : Excess cortisol, Exogenous or endogenous.
Tx : etomidate, ketoconazole, metyrapone, dx: 24 hr urine cortisol.
Pheochromocytoma:
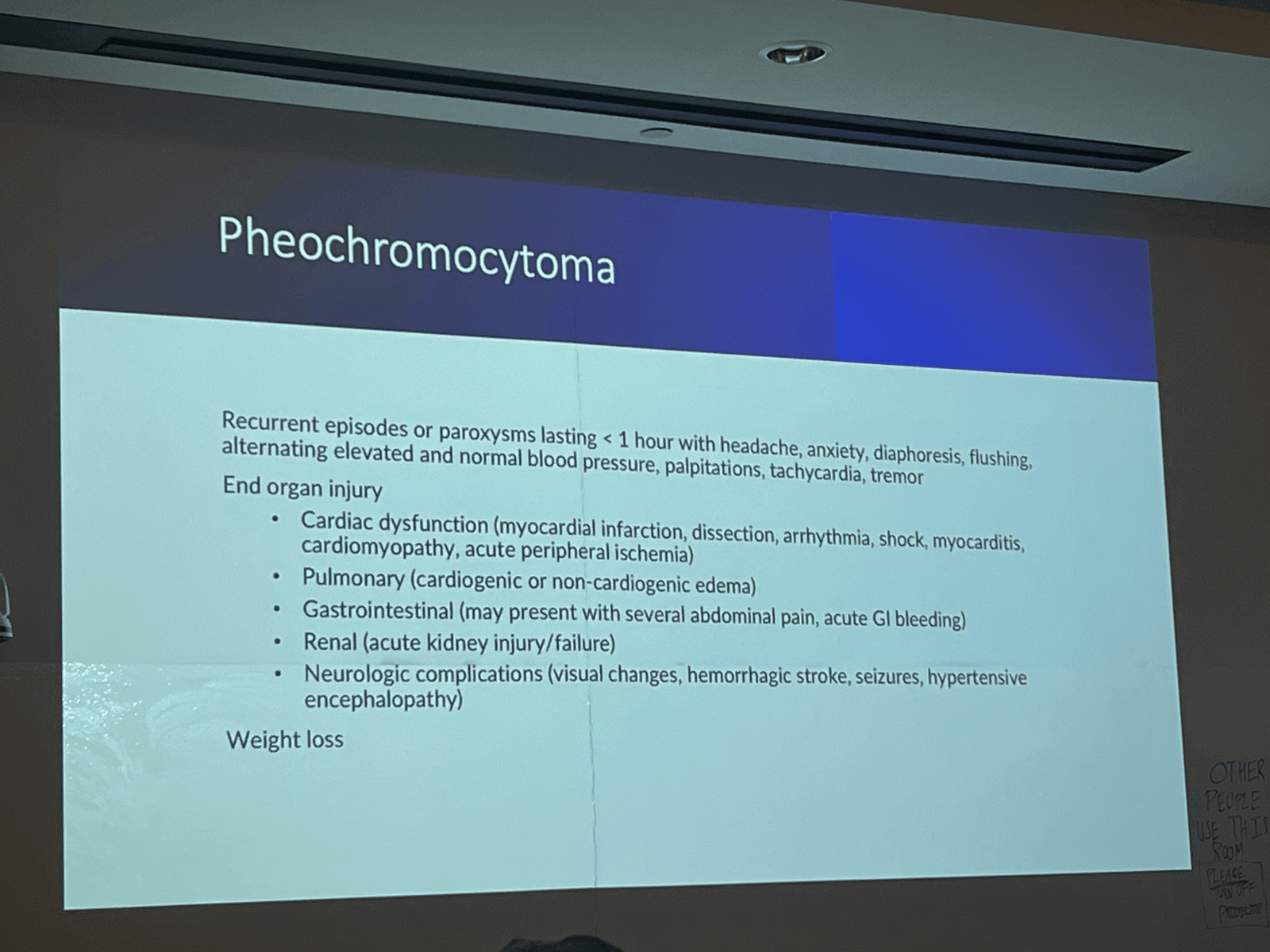
Dx, plasma free and fractioned metanephrines
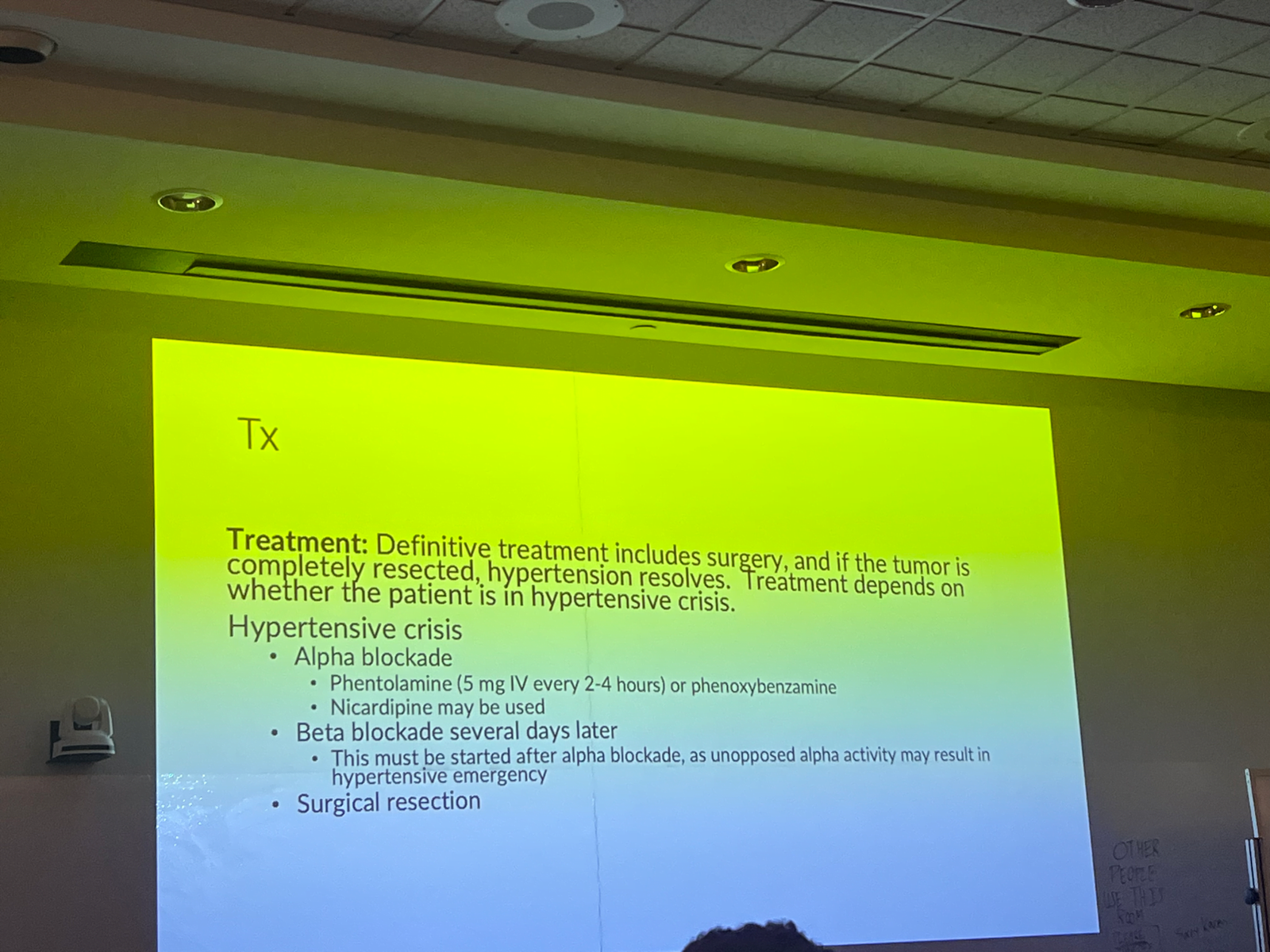
Tx :
Conn Syndrome : Potassium deficiency, htn
Kelly’s Presentation : ICH

Next Week- November 9, 2023
7:00am – 9:00am: Medical Education Grand Rounds. Laros Auditorium
9a – 12p: Education Center, Lecture Room 2
9)Teaching in overburdened systems – Rebecca Jeanmonod, MD
9:30) Thyroid Emergencies – Holly Stankewicz, DO
10) Endocrine Cases – multiple faculty
11) EM Case Presentation – Peter Gould, MD
11:30) TRIAGE – Chiefs
12) Optional board review – Brian Kelly, DO