When to worry and what to do with abnormal electrolytes – Guhan Rammohan, MD
- Hyper or hyponatremia
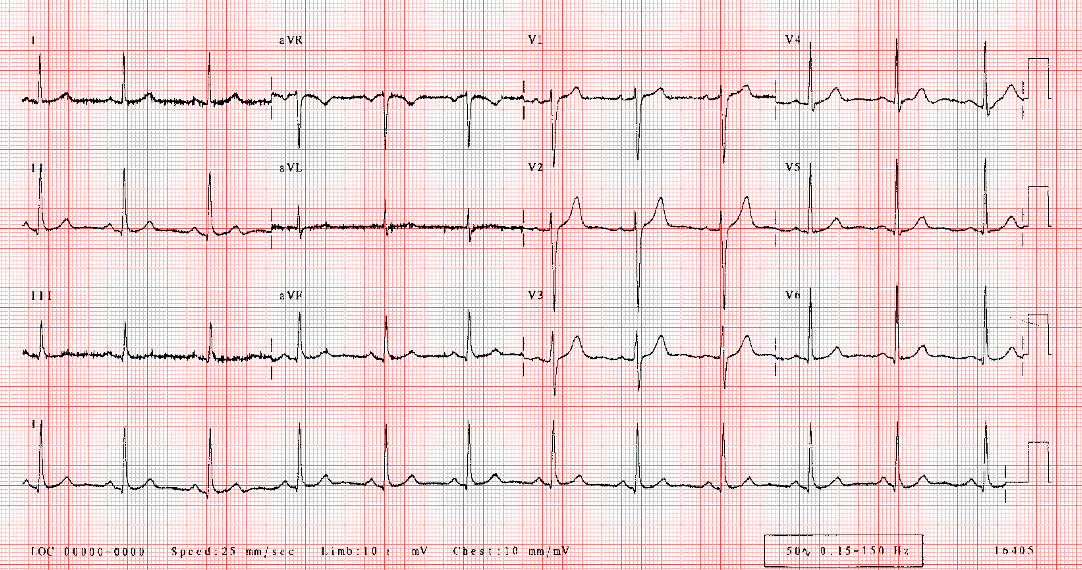
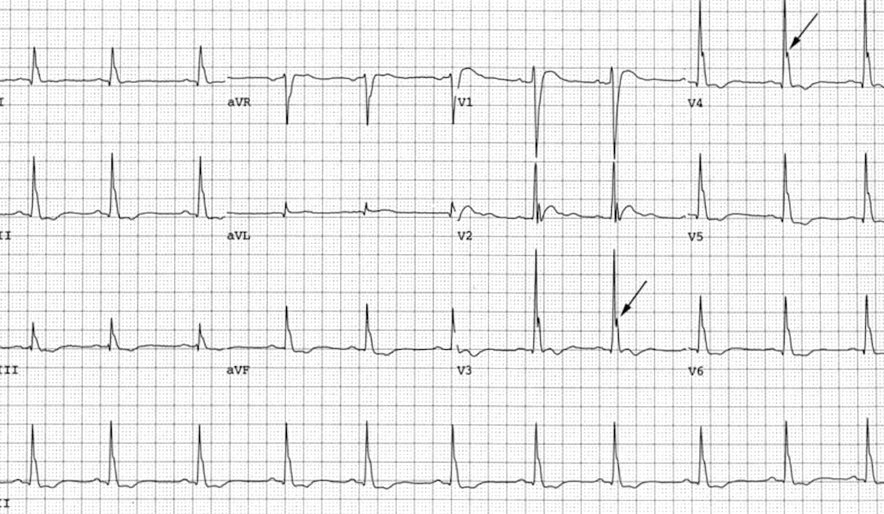
- Hyperkalemia = peaked t waves
- Hypocalcemia
- Prolonged QT interval due to ST segment prolongation
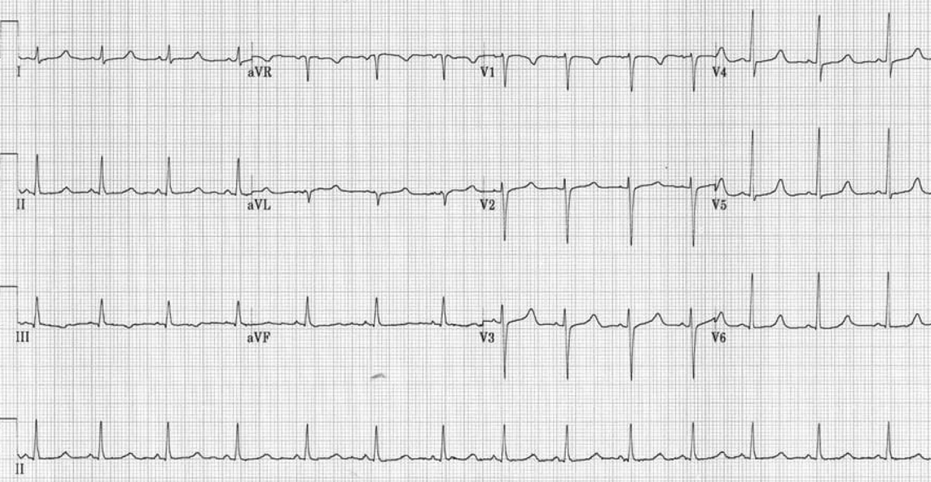
- Hypokalemia
- Prolonged QT interval with inverted t waves and U waves
- Hypomagnesemia
- Prolonged PR and QT intervals, T wave inversion, torsade’s

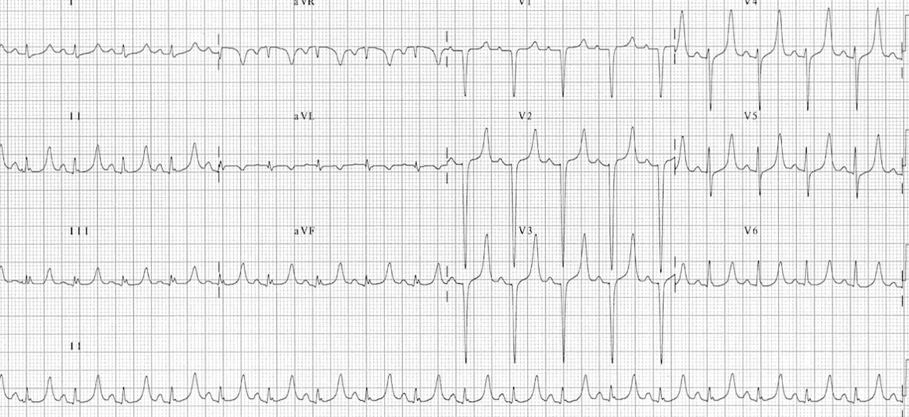
- Severe Hyperkalemia
- Peaked T waves with sine wave appearance
- Hypercalcemia
- Shortened ST segment and QT interval with J Osborn waves
-Hyponatremia
- How to calculate Osmolarity
- 2 x Na + glucose/18 + BUN/2.8
- Hypertonic Hyponatremia (Posm >295)
- Hyperglycemia, excess mannitol, glycerol therapy
- TX: NA containing fluids
- Isotonic Hyponatremia (Posm 275-295)
- “Pseudo”
- Hyperlipidemia and hyperproteinemia
- TX: none
- Hypotonic Hyponatremia (Posm < 275)
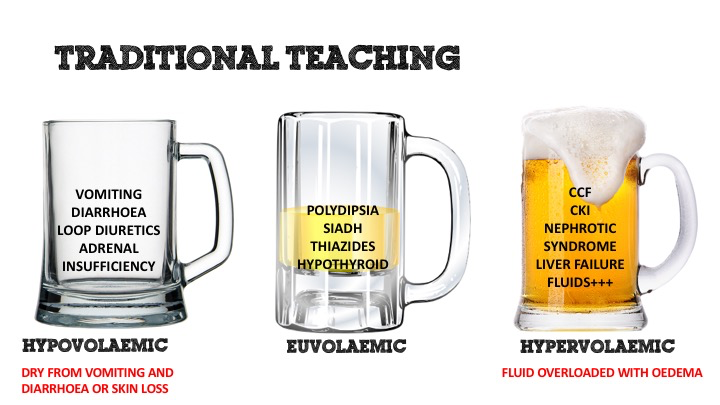
- Hypovolemic
- Renal
- Diuretic use, RTA, intersitial nephritis, osmotic diuresis
- Extrarenal
- GI loss, sweating, burns, pancreatitis
- TX: saline solution, hypertonic saline
- NA should be corrected at rate of 0.5 to 1 mEq/L per hour ( 12-24 mEq/L per day)
- If seizures present can increase to 1 to 2 mEq/L per hour
- DON’T CORRECT TOO FAST OR ELSE RISK FOR Osmotic demylenation syndrome
- Renal
- Euvolemic
- Urine NA >20
- SIADH; hypothyroidism drugs, psychogenic polydipsia ect
- TX: fluid restriction, salt tabs, vaptan durgs for SIADH
- Saline and hypertonic saline can be used
- Hypervolemic = looks overloaded
- Urine NA >20= renal failure
- Urine NA <20= cirrhosis, chf, nephrotic syndrome
- TX: treat underlying disorder + salt and water restriction
- Diuretics often used and sometimes dialysis
- Hypovolemic
- Hypernatremia
- Sodium above 150 due to decrease in total body water or increased salt intake
- TX: volume repletion
- Must calculate free water deficit
- TBW x [(measured Na/ normal NA) -1]
- TBW= BWkg x .60
- TBW x [(measured Na/ normal NA) -1]
- Once calculate free water deficit = replace half in the first 24 hrs
- If corrected too fast can cause cerebral edema
- Must calculate free water deficit
- Potassium: maintain at 4 or >
- 10mEq will raise the K+ by approximately 0.13mEq/L
- Ex. patient K 3.5mEq/L, to bring up to 4.0 patient will need approximately 40mEq of potassium
- IV options: KCl, KPO4
- Peripheral access 10mEq/1hr
- In ICU with central line and cardiac monitor: 20mEq/hr is fine
- IV if critically low or patient NPO
- If phos is low, can use KPO4 (especially in setting of DKA when patients may have low phos)—for each 3mmol/mL phos in KPO4, there is approximately 4.4mEq/mL in KPO4
- Oral options: KCl tablets or 10% KCl solution are options
- There is a KCl solution that can be used for PO patients with NG/OG tubes. If patient alert and tolerating PO, can use tablets
- >40mEq PO may cause GI upset
- 10mEq will raise the K+ by approximately 0.13mEq/L
- Hyperkalemia
- Cardiac manifestations are the most serious
- Mild K+ 6.5-7.5: tall peaked T waves, short QT interval, prolonged PR interval
- Moderate K+ 7.5-8: QRS widening and flat P wave
- Severe K+ 10-12: sine wave pattern
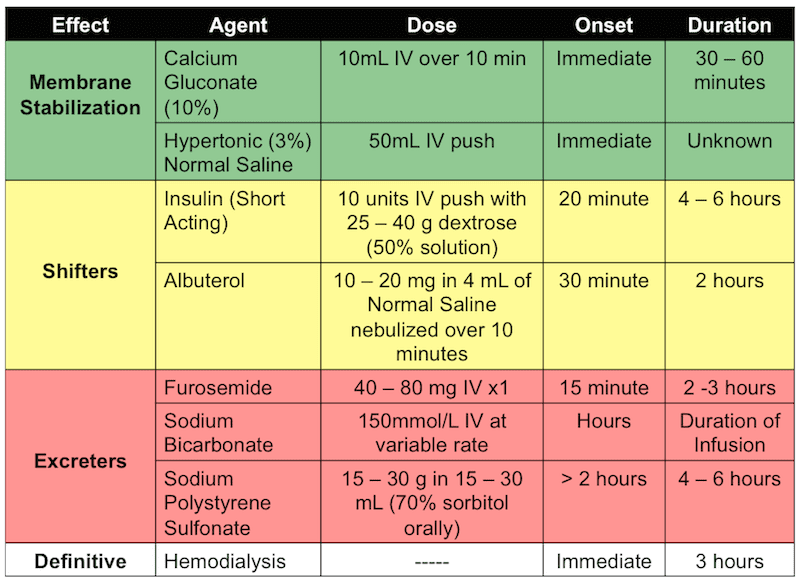
- TX:

- Cardiac manifestations are the most serious
- Calcium:
- Hypocalcemia= ionized calcium below 2.0 mEq/L

- TX:
- If pt is asymptomatic oral Ca therapy with or without Vit. D
- IV calcium can be given as CaCl or Ca gluconate but can cause vasoconstriction and is a vesicant
- In massive transfusion, CaCl can be given after every 4 to 6 units of blood if pt is in shock or heart failure
- Don’t forget that Magnesium needs to be replaced because of hypomagnesemia causing decreased release of PTH
- Hypercalcemia: ionized CA >2.7 or serum calcium above 10.5
- Tx:
- Initiate in any symptomatic patient with Ca above 14 mg/dL
- Involves volume repletion, increasing renal elimination, decreasing mobilization from bone, and correcting underlying disorder
- Aggressive IVF hydration to obtain urine output of 50-100 ml/hour, may use diuretics to enhance elimination if adequately volume repleted
- Bisphosphanates, calcitonin are effective in lowering calcium but not immediately and is not considered and ED therapy
- Tx:
- Mag
- Hypomag <1.5
- TX:
- Oral with Magnesium Sulfate, up to 6g/day
- The ER dose of IV Magnesium is 2g to 4g over 30 minutes-60 minutes
- Half of administered Mag will be excreted in urine
- Hypermag >3
- TX:
- Treatment is to stop intake of magnesium and IVF followed by furosemide can be given
- In severe cases CaCl can be administered and dialysis with decrease Mg bath
- Hypomag <1.5
- Phos
- Usually not a concern in the ED, but hypophosphatemia can be seen with treatment of DKA or alcoholic ketoacidosis and in the ICU with refeeding syndrome
- Hyperphosphatemia can be seen with Renal Failure patients and can be treated with phosphate binders
Cases in ED ultrasound: Trauma – Donald Jeanmonod
( Below are links to some great resources to go over fast exams )
http://www.mmheme.org/new-page-43
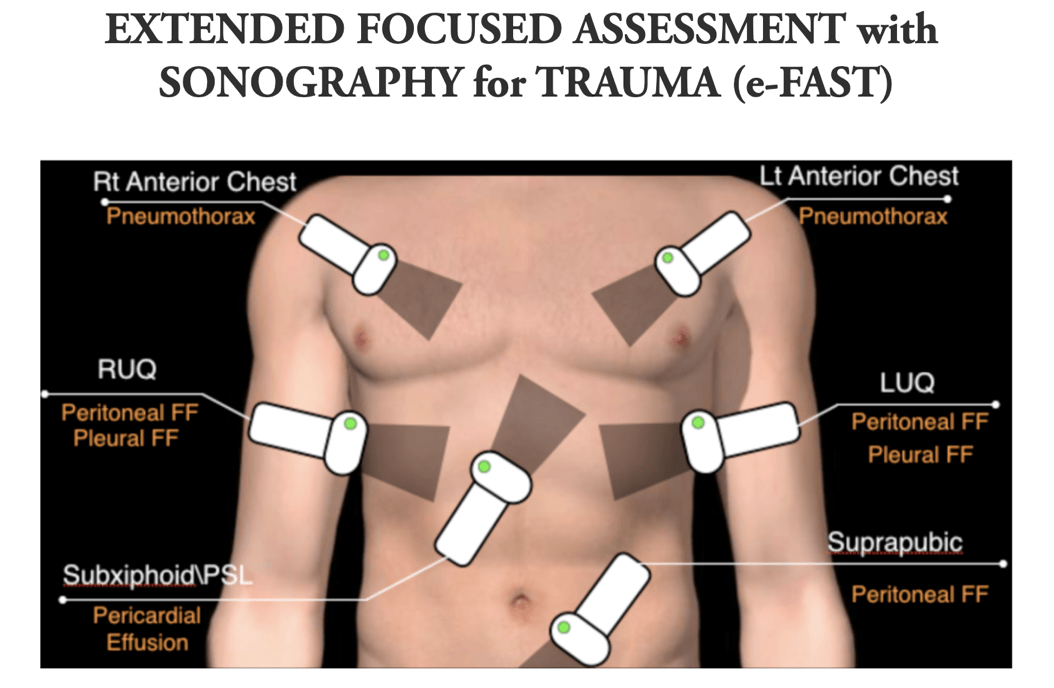
- FAST EXAM and what you’re actually evaluating!
- Cardiac (most often subxiphoid, but other views may be obtained):
- pericardium and
- heart chambers, especially the right ventricle
- Right Upper Quadrant (RUQ):
- Morrison’s Pouch (hepatorenal recess),
- liver tip (right paracolic gutter) and
- lower right thorax
- Left Upper Quadrant (LUQ):
- subphrenic space,
- splenorenal recess,
- spleen tip (left paracolic gutter) and
- lower left thorax.
- Pelvic:
- rectovesical pouch (male patients) or,
- in female patients, rectouterine / pouch of Douglas.

Interactive endocrine – Rachel Patterson, MD
Pictionary (:
Saves of the month(s) – John Pester, DO
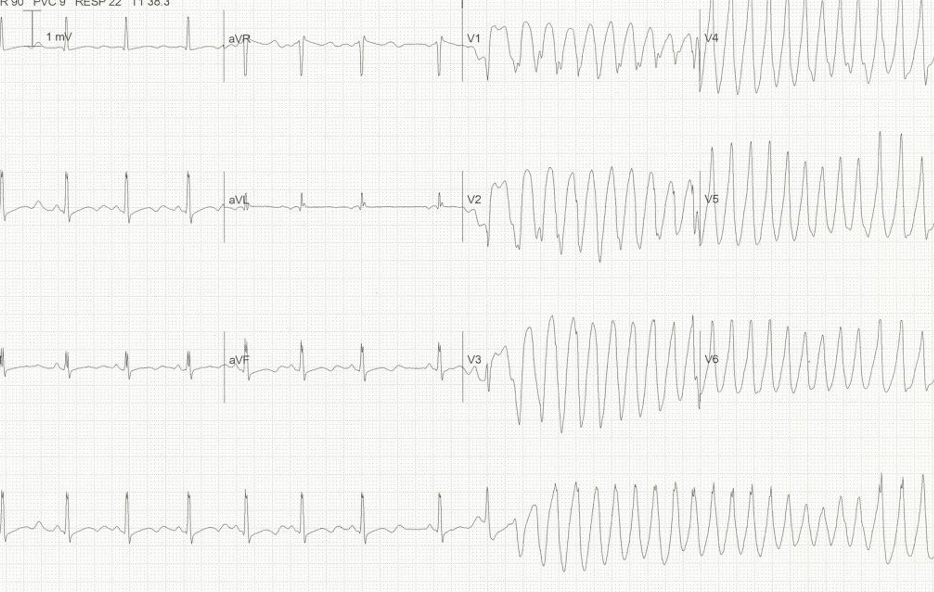
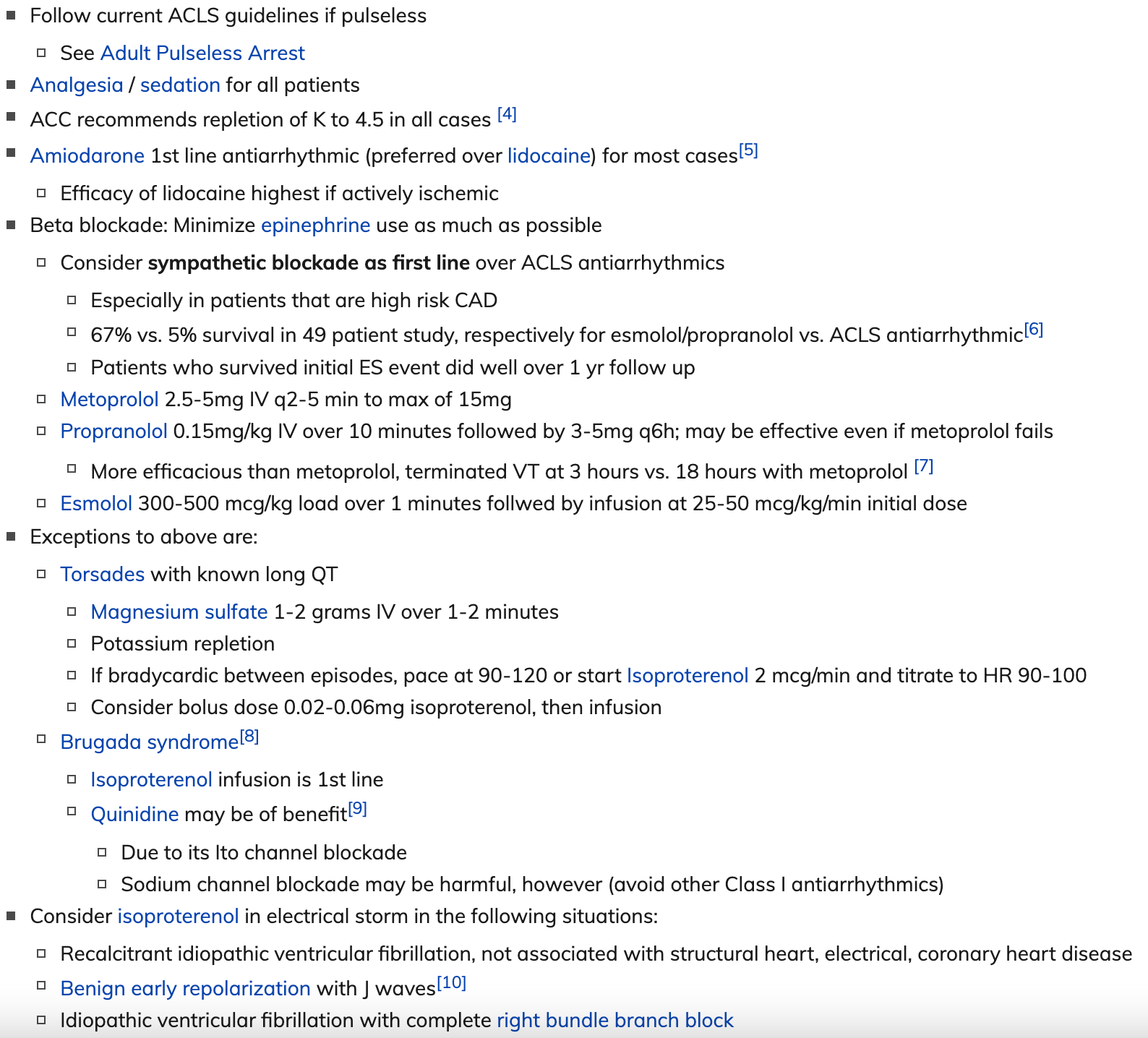
- Electrical Storm:
- Definition: 3 or more episodes of sustained ventricular tachycardia, ventricular fibrilation, or ICD shocks within 24 hours
- Most have underlying structural heart disease, but also seen in those with structurally normal hearts (i.e. Brugada syndrome, Long QT syndrome)
- What to do if you have a patient in Electrical storm?
TRIAGE – chiefs
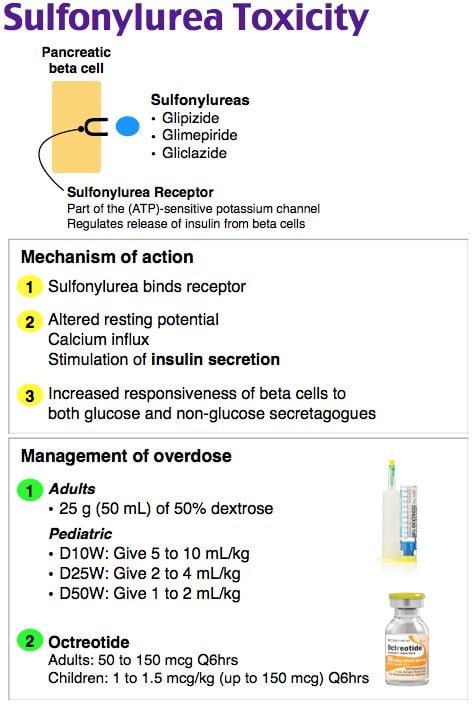
- Toxicology
- Radiology

- TX: pull on it and splint
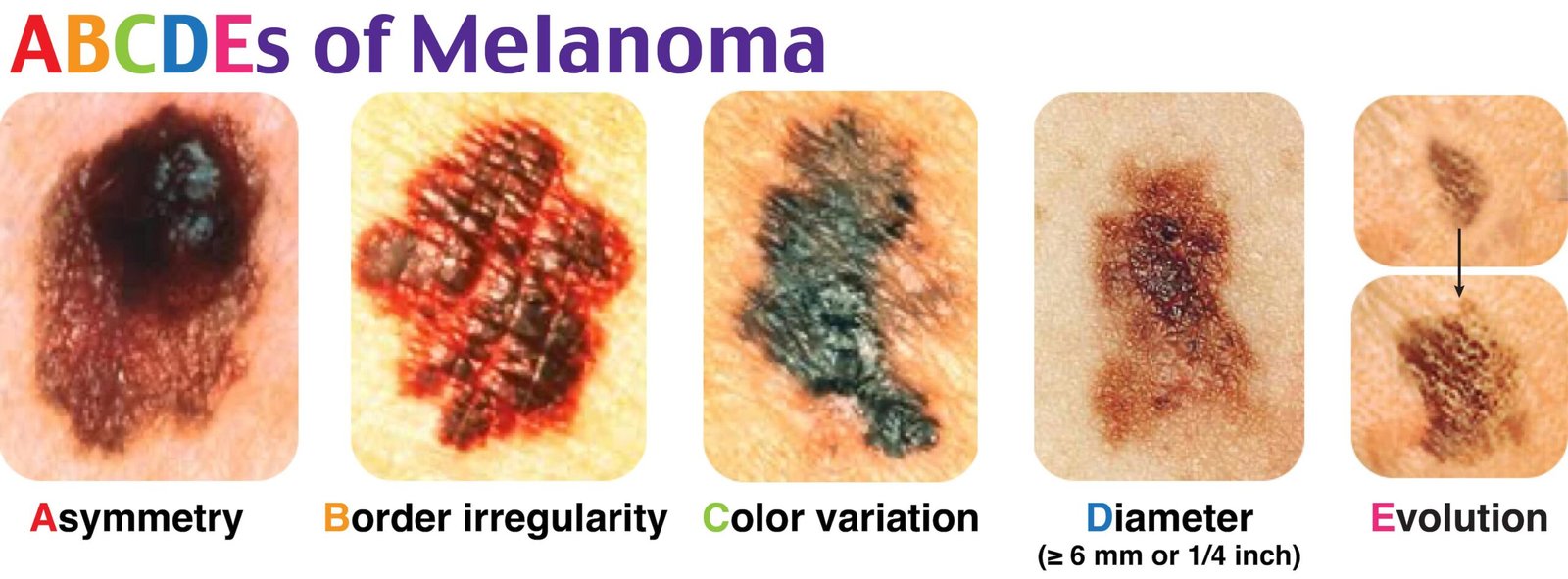
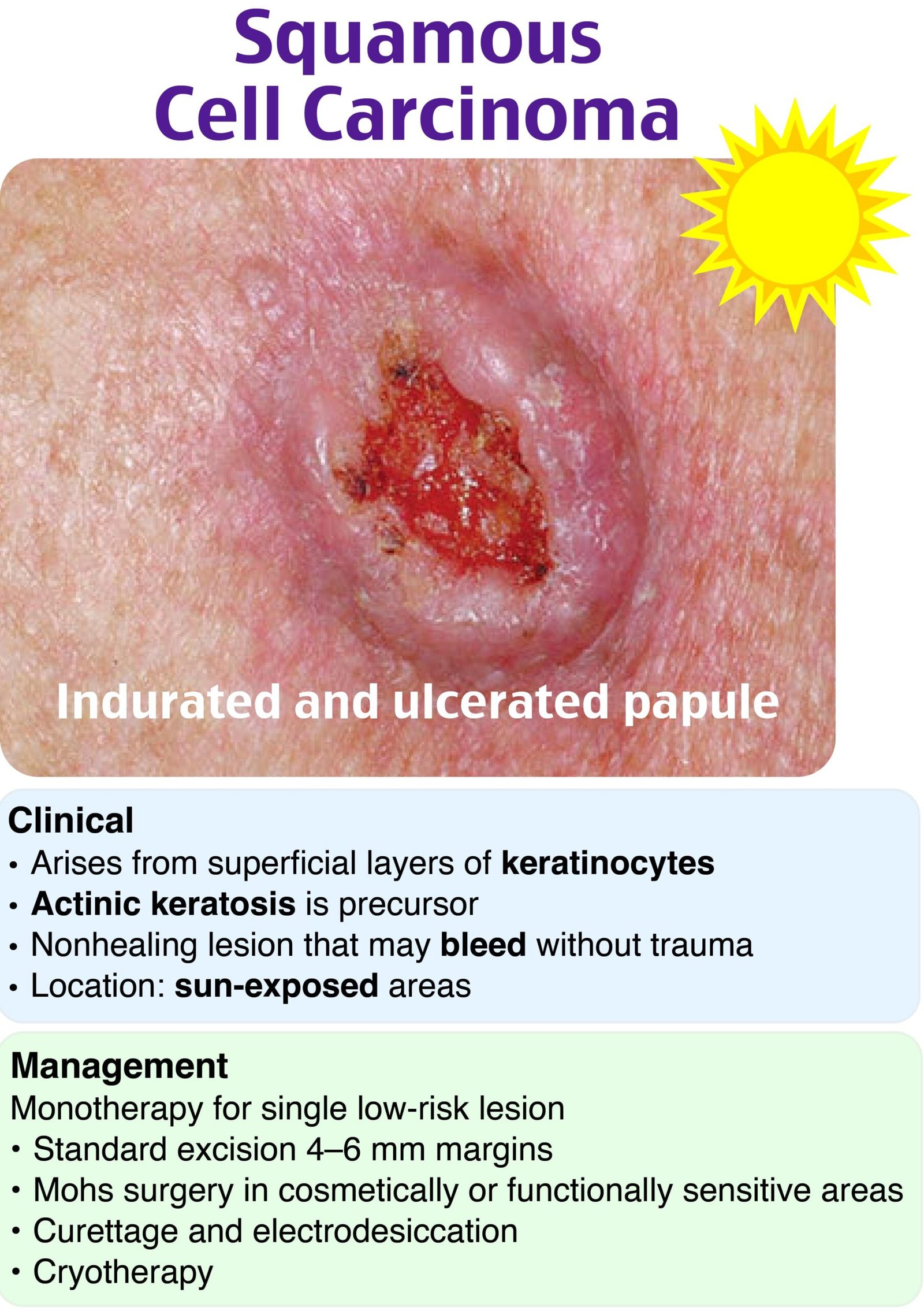
- Integument
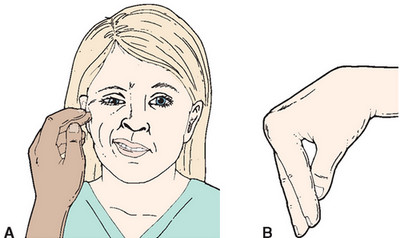
- Ancillary “Mothers Kiss”
- General
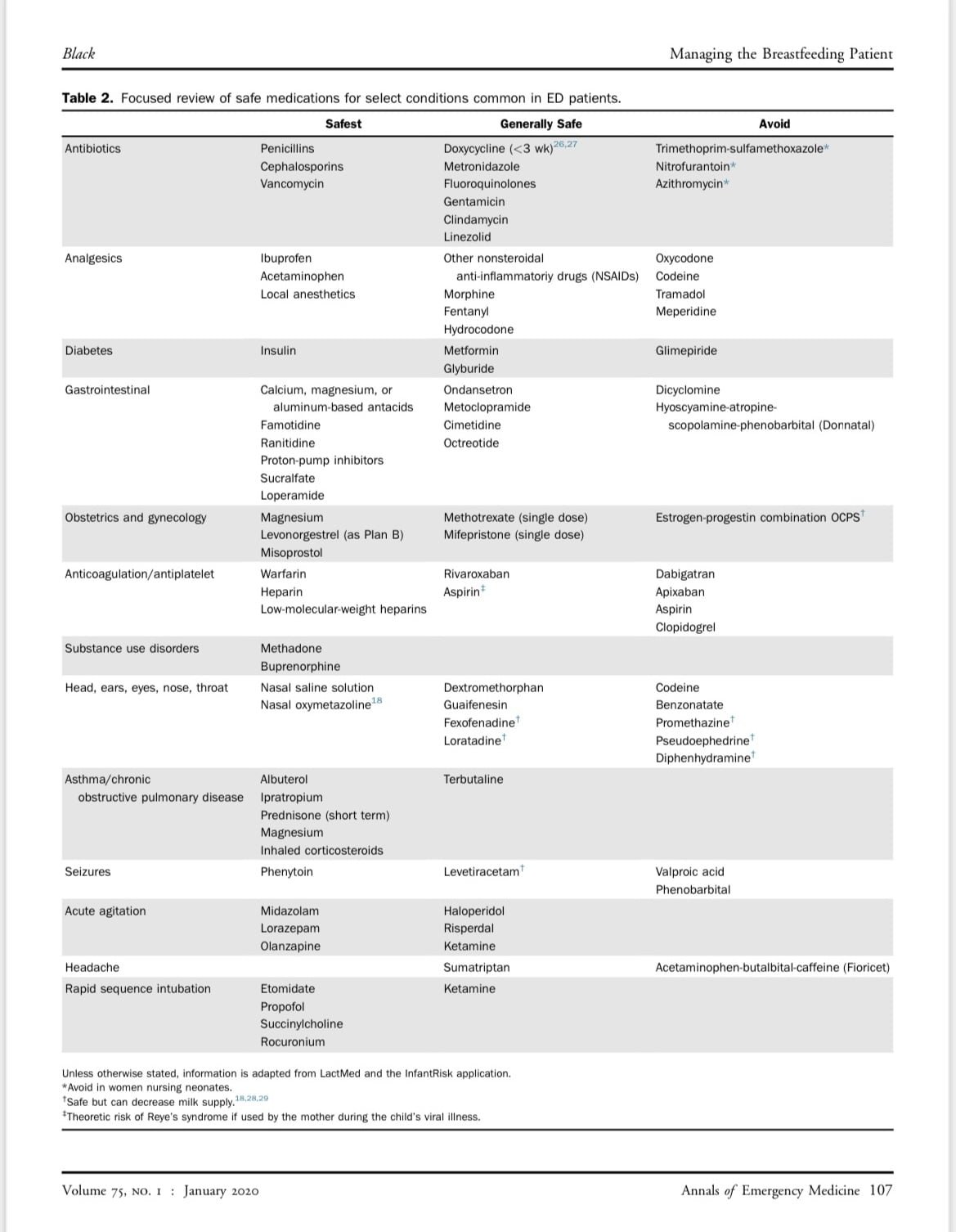
- Breastfeeding Dos’ and Donts when it comes to medications

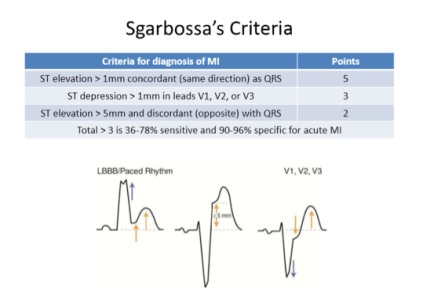
- EKG


Getting SUED- panel
- Attached document